International climate negotiations have long been haunted by a broken promise. In the wake of collapsed negotiations at the United Nations climate conference in Copenhagen in 2009, wealthy nations, led by the United States, pledged to provide developing countries with $100 billion in climate-related aid annually by 2020. The money was meant in part to ease tensions between the rich countries that had contributed the most to climate change historically and the poorer nations that disproportionately suffer the effects of a warming planet. But rich countries fell short of the target in both 2020 and 2021, deepening mistrust and stymying progress during the annual United Nations climate conferences, which are known by the abbreviation COP.
A new report from the Organization for Economic Cooperation and Development, or OECD, confirms what the international organization began to suspect just before last year’s COP28: that wealthy nations finally surpassed the $100 billion goal in 2022. And while they were two years late delivering on their promise, rich countries partially compensated for their earlier shortfalls, contributing nearly $116 billion in climate aid to developing countries in 2022, according to the latest data available. That additional funding helps fill the roughly $27 billion gap resulting from rich countries’ failure to meet the $100 billion threshold in each of the two years prior.
“If you underachieved in the first two years, overachieving in the rest of the period is a good way to make up for that, to make amends,” said Joe Thwaites, a climate finance expert at the Natural Resources Defense Council, a U.S.-based environmental nonprofit.
Even $100 billion, however, is far lower than the developing world’s estimated need. United Nations-backed research projects that developing countries (excluding China) will need an eye-popping $2.4 trillion per year by 2030 to transition away from fossil fuels and adapt to climate change.
Serious questions also remain about the quality and accounting of the existing funding. According to the OECD report, more than two-thirds of the public finance in 2022 was provided in the form of loans rather than no-strings-attached grants. That means developing countries are required to pay the money back, often with interest at market rates. A recent Reuters investigation also found that some aid providers required recipients to work with companies based in donor countries, meaning that much of the aid money ultimately found its way back to wealthy nations.
Such findings are likely to inform talks next week, as climate negotiators meet in Bonn, Germany, in preparation for COP29 in Baku, Azerbaijan, at the end of the year. Negotiators need to agree on a new collective goal for climate aid to developing countries this year. So far, different countries have submitted a range of proposals, with some nations floating $1 trillion annually as an appropriate number. Wealthy countries also want to expand their ranks so that some relatively rich countries that are technically classified as “developing,” like the oil-rich states of the Persian Gulf, can contribute funds toward the goal. Historically, only countries that the United Nations designated as “developed” in the 1990s have been on the hook.
The new OECD report’s findings may be advantageous to wealthy nations as they negotiate these thorny issues, according to Thwaites. “Developed countries were not necessarily arguing from a position of strength or moral high ground, having failed to meet the $100 billion on time,” he said. If countries continue to provide a similar level of funding for the next few years, they could make up for the shortfall. “Making up for 2020 and 2021, meeting the goal in those two years, could help rebuild a bit of trust,” Thwaites added.
The OECD report found that funding from all types of sources — multilateral development banks, the private sector, and public finance from governments — grew across the board in 2022. The increase in private-sector funding was particularly notable, jumping by more than 50 percent to a total of $21.9 billion.
The report indicated specific progress on funding for adaptation measures like sea walls and disaster-resilient infrastructure, an oft-overlooked area of climate finance. In 2021, countries pledged to double adaptation finance from the $19 billion provided in 2019 to $38 billion by 2025. According to the OECD report, adaptation funding had already risen to $32.4 billion one year after the pledge.
As in past years, loans continued to make up the majority of funding. While developing countries have called on wealthy nations to move away from loans as the primary form of aid, all parties seem to agree that loans can be appropriate in some circumstances. For projects that generate revenue — such as investments in renewable energy — loans tend not to have a detrimental effect because they pay for themselves. But for measures that don’t generate revenue — in particular, adaptation measures like sea walls — loans can trap countries in cycles of debt. As a result, the call for increasing grant-based funding has grown louder in recent years.
“A lot of countries are in debt distress,” said Thwaites. “And if they take on more loans for adaptation, where it doesn’t necessarily generate a return on the investment, that’s a challenge.”
Editor’s note: The Natural Resources Defense Council is an advertiser with Grist. Advertisers have no role in Grist’s editorial decisions.
Georgia Governor Brian Kemp called for more new nuclear energy at an event Wednesday celebrating the first new nuclear reactors built in the U.S. in decades, at Plant Vogtle near Augusta, Georgia. The construction of those reactors, known as Vogtle Units 3 and 4, cost more than twice its original budget and ended years behind schedule.
“Today, we celebrate the end of that project,” Kemp told the crowd of state officials and utility executives. “And now, let’s start planning for Vogtle Five.”
That could be a tough sell to Georgians who have seen their bills go up multiple times to pay for the new reactors and for shareholders of the power plant’s largest owner, who had to absorb some of the costs. Originally billed as the dawn of a new nuclear era and priced at $14 billion, the Plant Vogtle project was plagued by repeated delays and ultimately cost an estimated total of more than $31 billion.
When lead contractor Westinghouse filed for bankruptcy in 2017, prompting South Carolina to abandon its own nuclear project, Vogtle became the only new nuclear construction in the country. It still is.
“If building more nuclear were a good idea, other states would be jumping on the bandwagon now,” said Liz Coyle, executive director of the consumer advocacy group Georgia Watch. “The fact that they’re not, I think, speaks volumes.”
Coyle said her group is preparing to fight any proposal for another reactor.
For their part, the elected officials and utility executives at Wednesday’s event spoke of Plant Vogtle as a success story.
“Vogtle 3 and 4 don’t just represent an incredible economic development asset for our state and … a milestone for our entire country,” Kemp said. “They also stand as physical examples of something that I remind myself of every day: Tough times don’t last. Tough people do.”
Triumphal arrangements of the national anthem, “God Bless America,” and “Georgia On My Mind” backed by a gospel choir bookended the celebratory speeches. Attendees could snack on a sheet cake model of the power plant rendered in fondant.
A sheet cake version of the nuclear Plant Vogtle was among the celebratory aspects of the reactor’s opening ceremony.
Emily Jones / Grist
Speakers touted Plant Vogtle as a win for clean energy, since it can produce enough electricity to power a million homes and businesses without the greenhouse gas emissions produced by coal or gas, according to Georgia Power, which owns the largest stake in the new reactors. That carbon-free energy is key to attracting new businesses to the state, Kemp and others said.
All five members of the Georgia Public Service Commission, or PSC — which oversees Georgia Power’s planning and rates, including the Vogtle project — addressed the crowd.
“I just hope that we keep it up. We really should,” said commissioner Tricia Pridemore. “If we want to continue clean energy for our nation, it’s gonna take more than four.”
In December, the PSC approved a deal that hikes Georgia Power customers’ rates now that Vogtle Unit 4 is online.
After the Wednesday event, commissioner Tim Echols said he supports more nuclear power in Georgia, but said a further Vogtle expansion would need to come with protections against runaway costs and other problems that plagued the last project.
“I really need some protection against a bankruptcy,” he said. “I just can’t do it on the same basis again.”
Echols suggested a federal “backstop” and a mechanism to ensure large customers like factories and data centers would pay for the bulk of nuclear construction.
Under current Georgia law, a further expansion of Plant Vogtle would need to be financed differently than the project that just wrapped up, Coyle said. In 2018, state lawmakers approved a sunset provision for the state law that had allowed Georgia Power to pass Vogtle’s financing costs on to customers during construction. Barring another change, that would mean Southern Company and its shareholders would shoulder those costs.
Coyle said she’ll be urging lawmakers to keep it that way.
“Georgians are struggling, really, really struggling already to pay their power bills,” she said. “I hope we don’t have to go down this path again.”
On Friday, U.S. Secretary of Energy Jennifer Granholm and national climate advisor Ali Zaidi are visiting Vogtle for another event at the power plant. According to the Department of Energy, they plan to meet with local officials, as well as industry and labor leaders.
In a new study, researchers from the Institute of Neurobiology at Germany’s University of Tübingen have found that crows are able to learn to produce a specific number of calls, showing advance planning.
How many calls they will make can be predicted from the first vocalization in a sequence, a press release from University of Tübingen said.
“Producing a specific number of vocalizations with purpose requires a sophisticated combination of numerical abilities and vocal control,” the researchers wrote in the study. “We show that crows can flexibly produce variable numbers of one to four vocalizations in response to arbitrary cues associated with numerical values. The acoustic features of the first vocalization of a sequence were predictive of the total number of vocalizations, indicating a planning process. Moreover, the acoustic features of vocal units predicted their order in the sequence and could be used to read out counting errors during vocal production.”
Carrion crows are known for their impressive learning ability, which includes being able to count.
“In addition, they have very good vocal control. They can control precisely whether they want to emit a call or not,” said Andreas Nieder, a professor of animal physiology at University of Tübingen, in the press release.
The research team conducted behavioral experiments to see if three carrion crows could combine their ability to count with vocal control.
The corvids were given the task of producing from one to four calls that appropriately corresponded with specific sounds or an array of Arabic numerals, followed by pecking an enter key.
“All three birds succeeded in this. They were able to count their calls in sequence,” Nieder said in the press release.
The crows displayed a relatively long response time between when they were presented with the stimulus and their first call, which became longer as more calls were added. The delay’s length was not affected by the type of stimulus.
“This indicates that, from the information presented to them, the crows form an abstract numerical concept which they use to plan their vocalizations before emitting the calls,” Nieder explained. “Using the acoustic properties of the first call in a numerical sequence we could predict how many calls the crow would make.”
Some errors were detected in the birds’ calls.
“Counting errors, such as one call too many or one too few, arose through the bird losing track of the calls already made or still to be produced,” Nieder said. “We are also able to read out these types of errors from the acoustic properties of the individual calls.”
Being able to produce a deliberately chosen number of calls requires a sophisticated combination of vocal control and numerical competence.
“Our results show that humans are not the only ones who can do this. In principle it also opens up sophisticated communication to the crows,” Nieder said.
The study, “Crows ‘count’ the number of self-generated vocalizations,” was published in the journal Science.
A new report by scientists at Lawrence Berkeley National Laboratory and renewables consulting firm Clean Kilowatts has found that the United States’ increasing use of renewable energy has improved air quality and reduced the country’s greenhouse gas emissions while producing monetary benefits in the hundreds of billions of dollars.
For the data-based study, the research team focused on a surge in U.S. renewable energy use from 2019 to 2022, reported The Guardian.
“From 2019 through 2022, wind and solar generation increased by about 55%,” said Dev Millstein, lead author of the study and a research scientist with Lawrence Berkeley National Laboratory, as The Guardian reported. “By 2022, wind and solar provided roughly 14% of total electricity needs for the U.S.”
The researchers found that the country’s reduction in the use of fossil fuels, coupled with an increase in wind and solar, slashed its carbon emissions by 992.1 million tons — equal to taking 71 million automobiles off the road each year.
“Wind and solar generation reduce electric sector pollutant emissions and associated climate-related and air quality-related health damages,” the scientists wrote in the study. “From 2019 through 2022, wind and solar generation in the United States provided $249 billion dollars of climate and air quality benefits based on central estimates. In 2022, the normalized benefits were $143/MWh and $100/MWh for wind and solar, respectively, or $36/MWh and $17/MWh when only including air quality benefits. Combined, wind and solar generation led to 1,200 to 1,600 fewer premature mortalities in 2022.”
Air quality benefits from the use of renewables can eclipse major climate benefits, the researchers wrote. In order to bring the co-benefits to light, they quantified the amount of toxic air emissions reductions that were provided by wind and solar, with a specific focus on the fossil fuels nitrogen dioxide (NOx) and sulfur dioxide (SO2), reported The Guardian.
The team discovered that NOx and SO2 emissions — both associated with an increased risk of asthma and other health issues — had been reduced by 1.1 million tons during the study period.
To find out how much the reduction impacted public health, Millstein said they tracked the portion of the population that had been exposed to power plant pollution using air quality models. They also looked at disease research to determine emissions impacts and quantify the value of reducing the population’s risk of early death using a dollar value established by the U.S. Environmental Protection Agency.
The researchers also looked at the advantages of wind and solar in specific regions of the U.S. They found wind to be especially beneficial in Central states because of the displaced emissions on local power grids. The same was true of solar in the Carolinas.
“These findings can help us target future wind and solar development to provide the greatest climate and health benefits,” said Jeremiah Johnson, a North Carolina State University professor of climate and energy who was cited in the study, as The Guardian reported.
Johnson hopes the research will help people pay attention to the benefits renewables are already providing.
The public “is often focused on the challenges we face” as far as ecological damage goes, Johnson said. “But it is also important to recognize when something is working.”
With all eight native freshwater turtle species of Ontario considered at-risk, researchers have created protective nests to help boost offspring survival.
Researchers at the University of Waterloo and McMaster University designed a nest with materials like moss and lichen to mimic the turtles’ natural rocky nesting sites. As the research team pointed out in their study, published in the journal Restoration Ecology, previous nest restoration efforts often focused on building nests from materials like sand and gravel.
Examples of nest sites created with moss (A), mixed materials (B) and lichen (C). Restoration Ecology
The team instead focused on designing a nest that would work best for rocky landscapes, where freshwater turtles often create their nests in the cracks of rocks. Plus, they pointed out in their study that the mound nests made with sand and gravel tend to require regular upkeep to prevent plants from growing too densely into the nesting areas.
The researchers created the first nest for a research site at Georgian Bay in 2019 and monitored it for five years. During this time, the researchers didn’t need to make any repairs or adjustments to the nest they created, meaning it could be a low-maintenance way to help with freshwater turtle protection efforts.
A Blanding’s turtle at its new nesting site. Hope Freeman / McMaster University
While freshwater turtles can make their own nests, these efforts are often set back as the animals face threats from habitat destruction.
“The number 1 threat to freshwater turtles in Ontario is habitat loss and degradation from urbanization,” Chantel Markle, the lead author of the study and professor in the Faculty of Environment at the University of Waterloo, said in a press release. “Georgian Bay is one of the last remaining strongholds for some at-risk turtles in Ontario, so this new design is a step towards the survival of the species.”
Additionally, freshwater turtle eggs depend on certain temperatures to produce male or female hatchlings, and too many males or females can limit the reproduction of offspring in future generations, further threatening the survival of at-risk species. So the researchers took extra care to create warm, well-draining nests that would give the offspring the best odds of survival as well as hopefully improving population size in the long-term.
“Taking an interdisciplinary approach to assessing the success of habitat created for animal reproduction is critical,” Markle said. “In this study we evaluated the physical, ecohydrological and ecological success of the created nesting habitat — a combination not often seen in a single study.”
The team found that the eggs were 41% likely to hatch in the human-crafted nests, while the natural nesting sites only had a 10% chance for eggs to hatch.
Next, the researchers plan to scale the nest design to apply to other local, rocky landscapes. Additionally, they made their nest creation process available in the published study to aid turtle conservationists in other areas throughout Canada and the U.S.
International climate change panels often point out that women are more vulnerable to climate change than men. Hotter temperatures and more volatile weather inflame existing gender-based vulnerabilities, like domestic violence, inadequate access to health care, and financial insecurity. But there is another, largely invisible layer of climate impacts that falls along gendered lines: Research shows that climate change takes a profound physical toll on bodies that can bear children — from menstruation to conception to birth.
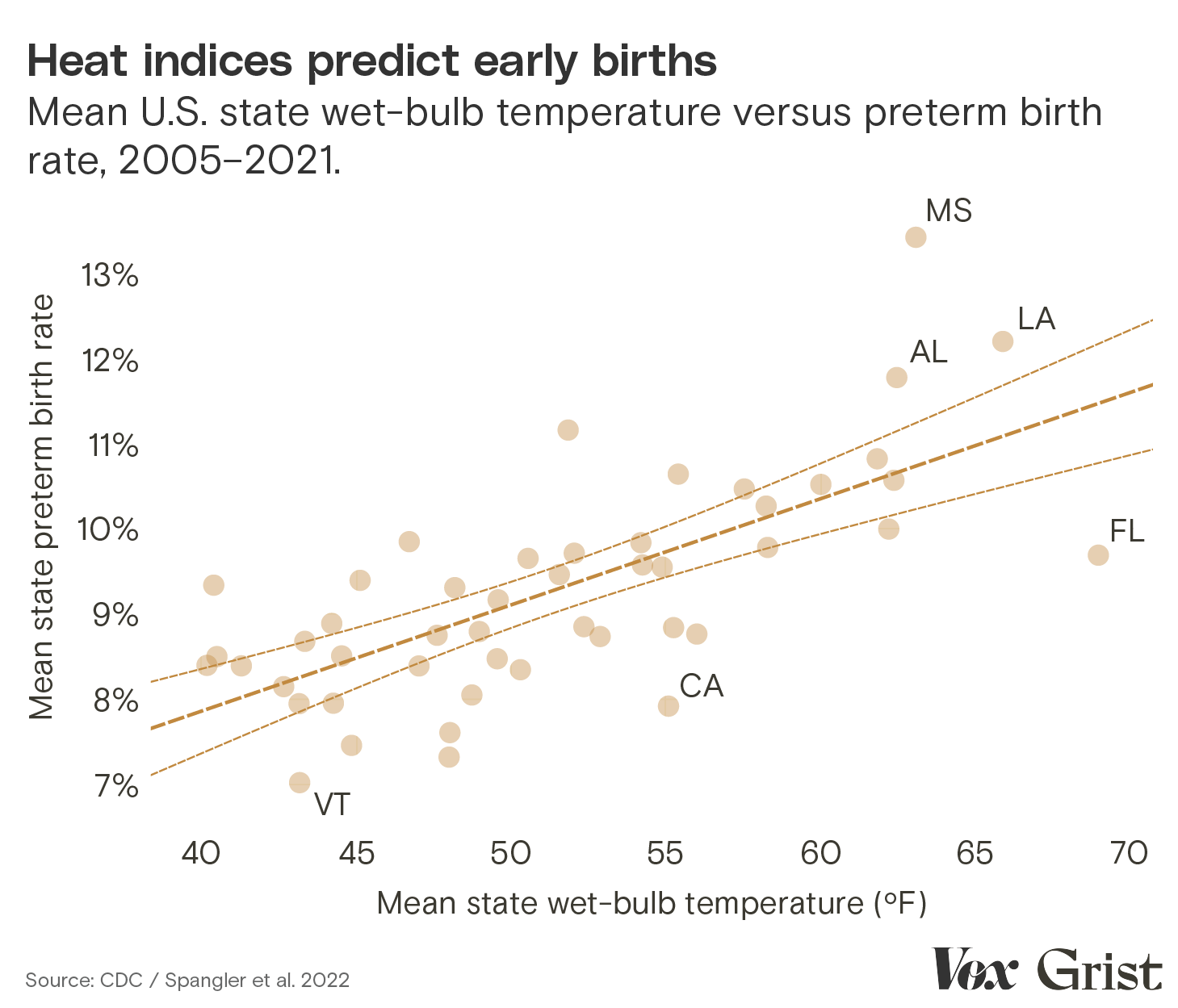
There are various pathways by which climate change worsens health problems before, during, and after pregnancy. A pregnant person’s immune system stands down during those crucial nine months so as not to reject the growing fetus, leaving the gestating parent more susceptible to climate-driven infectious diseases like malaria. Exposure to extreme heat during pregnancy increases the likelihood of preterm birth, although the biological mechanism behind this relationship is still poorly understood. Sea level rise infuses drinking water with salt, which can lead to high blood pressure — a risk factor during pregnancy for premature birth and miscarriage. And for those who have access to fertility treatment, which involves highly time-sensitive procedures, increasingly massive and intense storms are making assisted conception unpredictable.
Salt in the womb: How rising seas erode reproductive health
Women in Bangladesh are confronting the dangerous health effects of consuming salty water. They won’t be the last.
After years of neglecting to study the climate-related health conditions that affect women and gender minorities who can get pregnant, the medical establishment is just beginning to understand the scope of these threats. At a moment when reproductive autonomy is under political attack, climate change is making it even more dangerous to have a uterus.
Here, you’ll find a package of stories that will help you understand a few of the profound effects warming has on people who can get pregnant. The full range of climate-related reproductive threats is vast, and this series doesn’t touch on all of them. Instead, it provides a series of snapshots — four windows into the lives of women who are facing unexpected risks as they attempt to conceive, gestate, and give birth to children in a warmer world. Their stories are a warning to us all. —Zoya Teirstein
Credits
WRITERS | Zoya Teirstein, Virginia Gewin, Jessica Kutz, Mahadi Al Hasnat
STORY EDITORS | L.V. Anderson, Paige Vega, Kara Platoni
MANAGING EDITOR | Jaime Buerger
ART DIRECTION | Teresa Chin
ILLUSTRATIONS | Amelia K. Bates
DATA VISUALIZATION | Clayton Aldern, Jasmine Mithani
COPY EDITORS | Claire Thompson, Joseph Winters, Kate Yoder
FACT CHECKERS | Sarah Schweppe, Melissa Hirsch, Caity PenzeyMoog
On their very first date, Kirsti and Justin Mahon talked about wanting kids. They met on a dating app in 2016, nine months after Kirsti moved from Texas to Florida. Almost immediately, they fell in love.
A little over two years later, they got married. Six months after that, they started trying for a baby. To their surprise, they got pregnant right away. But just as quickly, they had an early miscarriage. At 27, Kirsti didn’t have any reason to suspect fertility problems, and her obstetrician was quick to reassure her: Kirsti’s blood work looked normal, and getting pregnant after a month of trying is a good sign of fertility. Conceiving again, she was told, would be easy.
Over the next two years, Kirsti got pregnant three more times. None of her pregnancies lasted beyond the first trimester.
“It felt like we were hitting a brick wall,” Kirsti said. In January 2022, the couple went to see a fertility specialist who conducted a series of intensive tests that uncovered what was really going on. Kirsti was only 29 years old at the time, but the specialist told her that her egg quality was that of a 40-year-old’s. In vitro fertilization, or IVF, the specialist said, was Kirsti and Justin’s best hope.
A photo Kirsti Mahon posted to social media after her third pregnancy loss in September 2021. Courtesy of Kirsti Mahon
It didn’t take the couple long to decide to take the plunge. “With every loss that we had it was like I was watching Kirsti lose a piece of herself,” said Justin. “It became obvious with the consultation that the IVF process was really the only way to guarantee that this really brutal cycle wouldn’t continue.”
So they drained their savings, cashed in an old retirement account, and took out two loans to pay for the treatment. They live in Florida, a state where coverage isn’t mandated, so most of the procedures would be out of pocket. Justin estimates it cost between $25,000 and $30,000. The couple hammered out the minutiae of IVF with their specialist, down to the timing of every hormone shot. They felt ready.
But Kirsti and Justin hadn’t accounted for hurricane season.
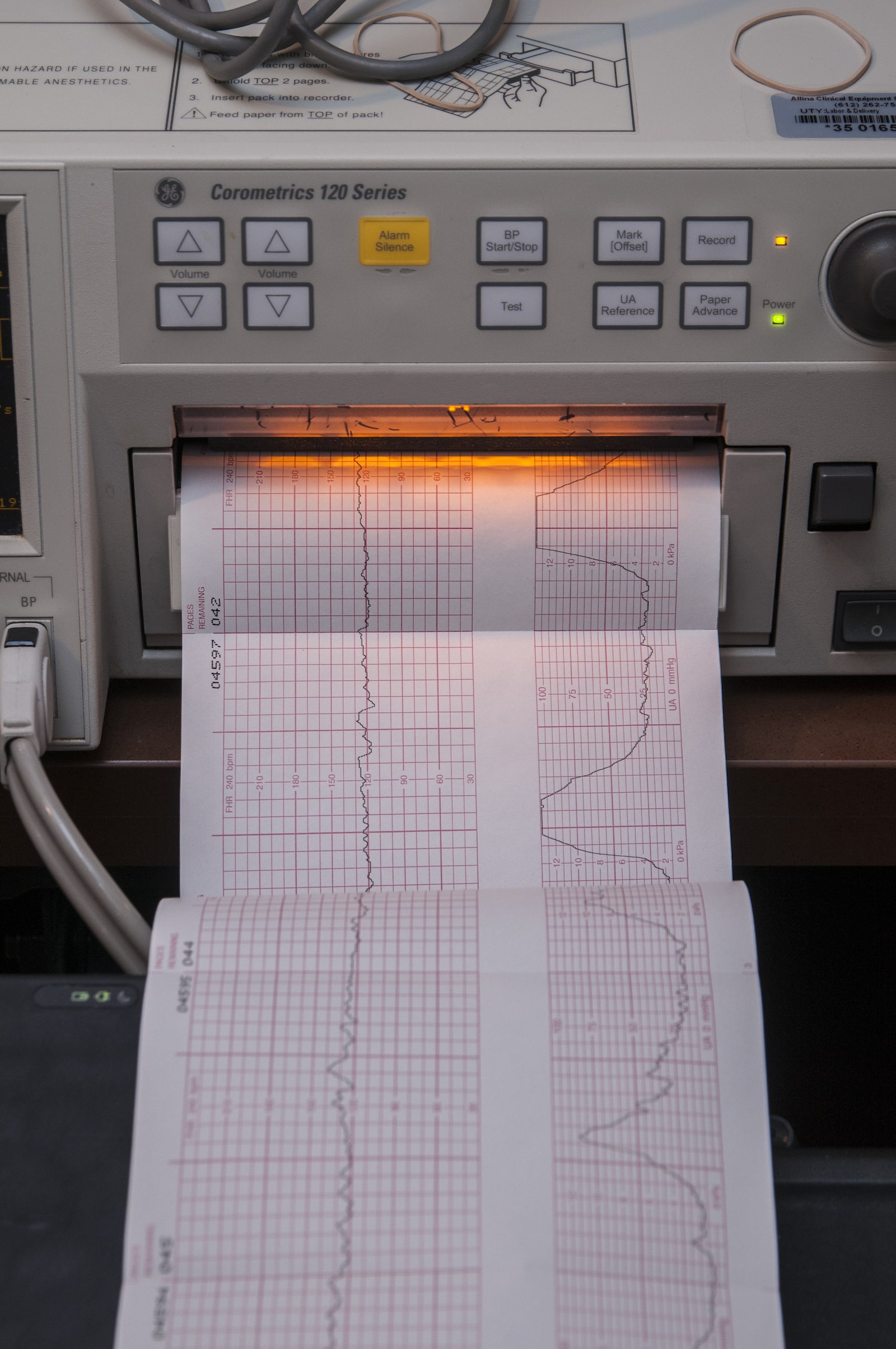
If the process of getting pregnant naturally feels murky and unpredictable, in vitro fertilization turns conception into a science — every menstrual phase, reproductive hormone and embryo carefully screened, tested, and optimized. First, patients inject themselves with fertility hormones aimed at stimulating ovarian follicles and bringing as many eggs as possible to maturity. An IVF cycle can fail right then and there, with the bad news showing up on an ultrasound screen or on the printed pages of a laboratory test before the eggs are even collected. Often, too few follicles develop. Ovulation can happen prematurely, or the ovaries can become hyperstimulated, causing pain, nausea, or more serious health problems. Everything can go wrong, and everything — down to the timing of each hormone shot — needs to go right.
If it does, the patient’s eggs are removed for fertilization in an outpatient procedure called an egg retrieval. The eggs must be harvested 34 to 36 hours after the “trigger shot,” a final hormone injection which prompts the eggs to finish maturing, but before the ovary releases them into the fallopian tubes. Patients are administered a painkiller, then the doctor guides a needle through the vagina or stomach and into the ovaries, aiming to suction all the eggs from their follicles. Mature eggs — there can be dozens, just one, or none at all — are fertilized with sperm in vitro, Latin for “in the glass,” or in this case in a petri dish. There, the embryos mature for three to six days. Not all of them survive, or develop correctly. The ones that make it can be reinserted into the uterus right away or, more commonly, frozen for later use.
Amelia K. Bates / Grist
Two time-sensitive procedures bookend the most stressful and critical weeks of the IVF process. The first is the egg retrieval. Once the trigger shot has been administered, there’s no turning back. If the procedure doesn’t take place approximately 36 hours after the injection, the patient’s follicles rupture, casting the precious eggs irretrievably into the fallopian tubes. A missed alarm, a traffic jam, or a delayed flight can wreck an enormous financial and emotional investment.
The second is the embryo transfer. A patient’s uterine lining must be sufficiently thick when an embryo is reinserted — otherwise, the embryo won’t implant, and the patient won’t get pregnant. Doctors often prescribe additional hormone injections for up to 12 weeks to boost estrogen levels and thicken the uterine lining before a frozen embryo is thawed and transferred. Fertility clinics typically require patients to come in regularly for ultrasounds to determine the optimal day for the transfer. If the lining remains too thin, or if the patient’s menstrual cycle advances too far, then the transfer must be delayed for at least another month.
These windows of opportunity are narrow, and it doesn’t take much to slam them shut. For a growing number of would-be parents living in the coastal areas of the United States, where climate change is making hurricanes faster-moving and more intense, all it takes is a single storm.
In September 2022, the Mahons were preparing for the final stage of IVF: the embryo transfer.
Kirsti had already undergone the grueling egg stimulation and retrieval process, which produced 23 eggs. Four had turned into embryos, and three were genetically tested. Two came back healthy and had been frozen.
A photo the Mahons posted to social media in February 2022. Courtesy of Kirsti Mahon
Her transfer had initially been scheduled for August, but it got canceled when Kirsti contracted COVID-19 that July. Now, as summer turned to fall, Kirsti spent five weeks injecting herself with hormones at their home on the outskirts of Naples, Florida, where she worked as an animal supervisor at the area zoo. Naples sits on Florida’s Gulf Coast, about 40 miles north of the northern edge of the Everglades.
Less than a week out from her transfer, she was at the clinic for a final ultrasound and some blood work when she asked whether she should be worried about a coming storm she had seen on a weather forecast. She remembers the nurse telling her, “We’ll keep an eye on it, but I really wouldn’t worry about it.” At that time, the storm system still looked like it might miss Naples.
That Monday, Kirsti and her husband had grown increasingly worried, so they emailed the fertility clinic for an update. While they waited to hear back, they tracked Hurricane Ian on the news, watching as it made its way toward the U.S. “It just kept getting scarier and scarier,” Kirsti said.
Jasmine Mithani / The 19th / Clayton Aldern / Grist
On Tuesday, Kirsti went into work and started to evacuate animals from their outdoor enclosures. At this point, the hurricane began to veer toward southwest Florida, but was still expected to make landfall more than a 100 miles north of Naples, sparing her town. That afternoon, calls began to stream in from her parents and her in-laws, who lived along the Florida coast. It was decided that they should take shelter in the couple’s house. By that evening, Kirsti’s two-bedroom, one-bath house was suddenly packed with family and a menagerie of pets.
On Wednesday morning, Justin injected Kirsti with the last dose of her medication. Southwest Florida was flooding, and parts of the state were losing power, but they hadn’t heard anything from the clinic. Their appointment was supposed to be the next day. As far as Kirsti knew, the procedure was still on track.
Hurricane Ian was a prime example of a storm charged by climate change. It strengthened from a Category 3 into a Category 4 hurricane in under 24 hours. Ian is just one of several major hurricanes that have struck the southern and southeastern coasts of the United States in the past decade — regions that are particularly vulnerable to damage during the Atlantic hurricane season. In places like Florida, Louisiana, Georgia, Puerto Rico, and Texas, it’s becoming increasingly evident that communities and the infrastructure they rely on are ill-prepared for intensifying storms.
Hurricane Ian intensifies as it heads toward Florida on September 26, 2022.
NOAA
Hurricane Harvey, a Category 4 storm that hit Texas in 2017, submerged hundreds of roads, collapsed bridges, and damaged more than 300,000 homes. That same year, Category 4 Hurricane Maria decimated Puerto Rico’s aging power grid, plunging the island into darkness for nearly a year — the longest power outage in U.S. history. In 2020, Category 4 Hurricane Laura barreled into southwest Louisiana, displacing thousands of residents and nearly destroying the city of Lake Charles. The city was still clearing wreckage caused by Laura, the most powerful storm to hit southwest Louisiana since record-keeping began, when another hurricane, Category 2 Delta, carved a nearly identical path of destruction through the state. Lake Charles continues to recover four years later.
Fertility clinics are just as vulnerable to storms as any other infrastructure. When Hurricane Ida hit New Orleans in 2021, Nicole Ulrich, a doctor at Audubon Fertility Center, experienced firsthand the challenges intensifying hurricanes pose to these centers. Similar to Hurricane Ian, Ida progressed so rapidly that it caught the city and clinic off guard.
Forecasters “thought it was maybe going to be a [Category] 1 or a 2, and then it was going to be a 3, and then all of a sudden, it was going to be a 4. At that point, there really should have been a mandatory evacuation, but there wasn’t enough time,” said Ulrich. “We had to close the clinic at that point, because there just wasn’t another option.”
As a result, Audubon had to cancel at least 10 IVF cycles, and delay the start of several others. This included patients who were preparing for embryo transfers, and others who had started injecting the hormones needed for egg retrieval. The clinic also had some embryos growing in the lab. It usually takes five or six days to tell which embryos are healthy and suitable for freezing, but Ulrich’s clinic had to quickly decide to freeze them early, on days two and three instead, just in case their backup power generator failed.
Once the clinic was back up and running, it took months before Ulrich and her team could fit in all the patients whose cycles had been canceled or delayed — patients who were anxiously awaiting the chance to restart the process.
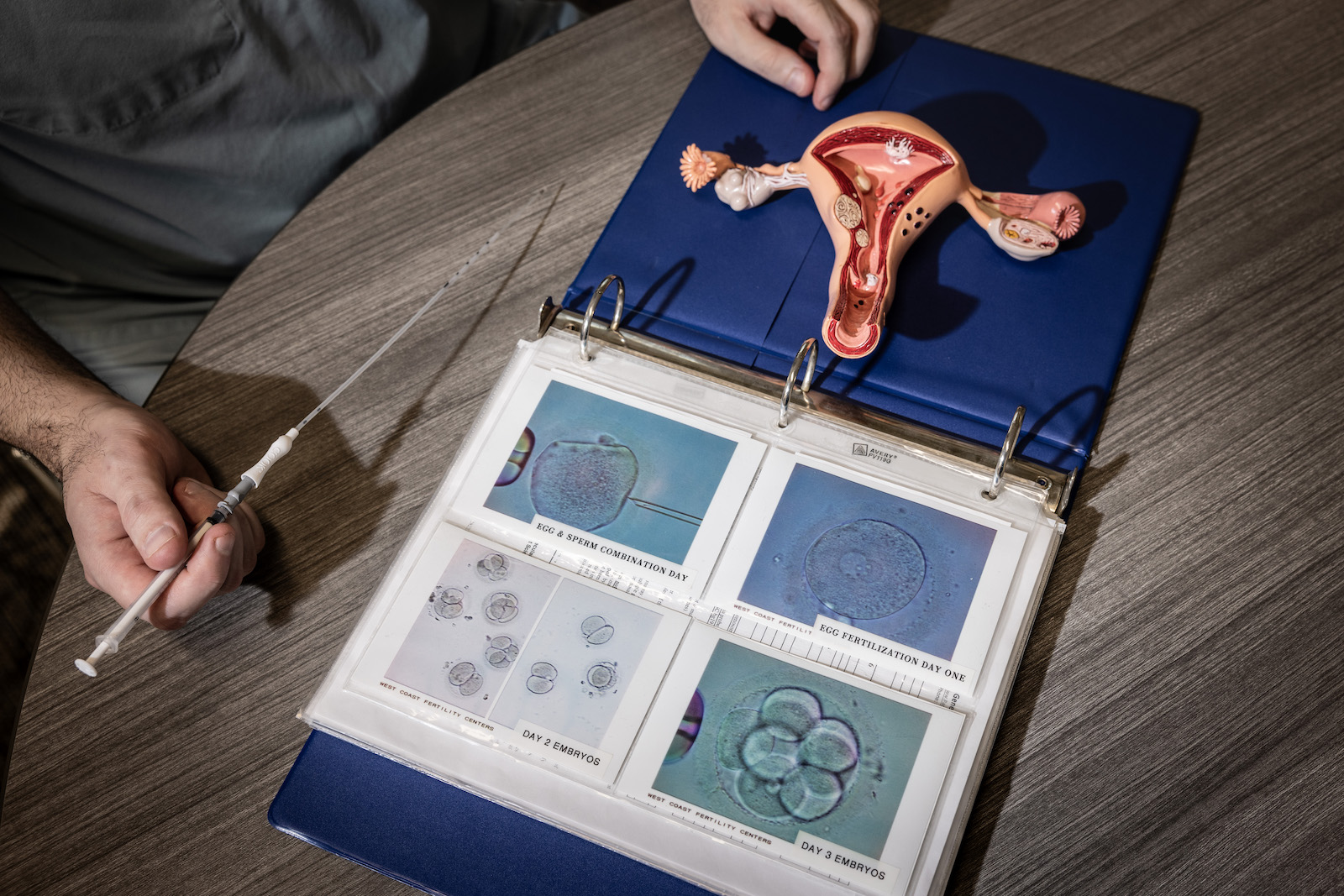
An embryo transfer catheter and a model of a uterus are displayed in a fertility clinic in California. Jay L. Clendenin / The Washington Post via Getty Images
“For most people, waiting a month is not going to make that big of a difference. But when you’re in that moment and you’re 42 and you know your egg count is low, it feels like just the most devastating thing that could happen,” said Ulrich. “There is a chance that, especially when you get closer to 43, it might make a difference.”
The embryos Audubon froze early had to be thawed in order to mature and then refrozen. The clinic is still analyzing data from that change in protocol to understand if it affected pregnancy outcomes.
Thanks to that experience, Ulrich published a paper in 2022 that calls for more research on the topic of IVF and climate change, with a focus on the particular challenges posed by rapidly intensifying hurricanes. “It had a huge impact on our clinic and our patients, and for months afterwards, we were still dealing with the aftereffects,” she wrote.
But the experience taught Ulrich lessons other IVF facilities could benefit from. Ulrich said she’d love to see clinics establish better relationships with other fertility treatment centers in their region so that patients could transfer to them in times of disaster. She also encourages clinic staff to review their emergency action plans to ensure they are prepared to meet the changing nature of storms, and to be ready to make decisions quickly to salvage cycles and protect embryos. All clinics store embryos in nitrogen tanks, which do not rely on electricity and are typically safe from blackouts or issues with electrical grids. But the labs that embryos mature in before they are frozen do depend on electricity — and if a disaster takes out power for too long, even backup generators can run out of fuel. During Hurricane Katrina, embryos were lost at one clinic for this reason.
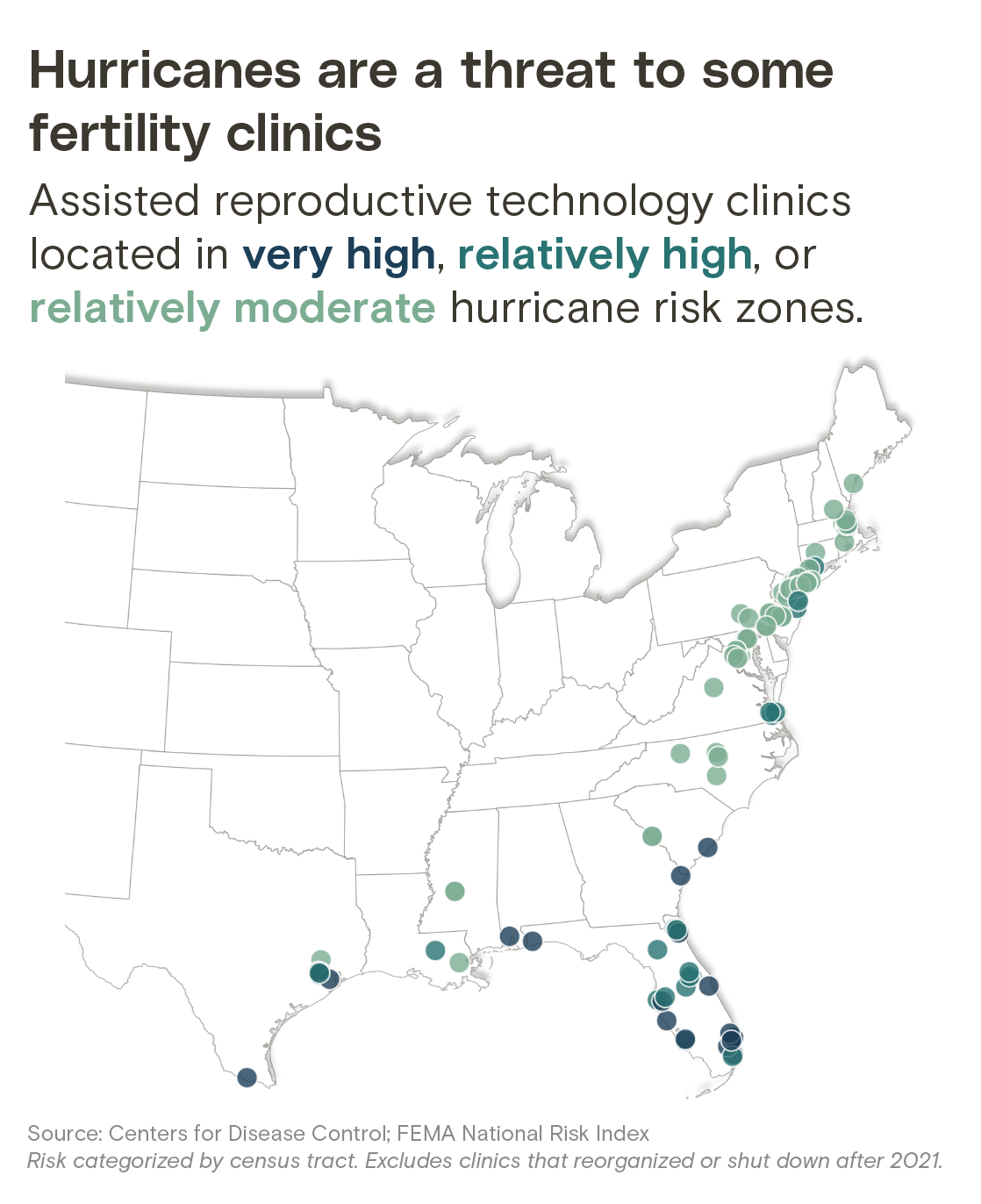
In 13 states, more than half of fertility clinics are at risk of hurricane damage
Share of assisted reproductive technology clinics in areas with “very high,” “relatively high,” or “relatively moderate” hurricane risk
State
Share of clinics in risky zones
Table displays only states with at least one clinic in a high-risk area. Risk categorized by census tract. Excludes clinics that reorganized or shut down after 2021.
Source: Centers for Disease Control; FEMA National Risk Index
Chart: Jasmine Mithani / The 19th; Clayton Aldern / Grist
IVF clinics are currently not required to have emergency plans in place, but it is recommended by the American Society of Reproductive Medicine. In 2022, the society published its own paper highlighting the need for clinics to adapt to increasingly threatening hurricane seasons.
“Clearly, climate change means you are having more extreme weather events, and [I] think that, like every other part of society, from homeowners to hospitals, fertility clinics have to think a bit more about how they can build more resilient systems,” said Scott Tipton, chief advocacy and policy officer with the American Society of Reproductive Medicine.
Within a few hours of Kirsti’s final hormone injection, she saw her nurse’s name light up on her phone. Before ducking into her bedroom to get some privacy from the houseguests, she exchanged a despairing glance with Justin. “I just looked at my husband and I was like, ‘It's not happening, it's not happening,’ and I took the phone call.”
The nurse immediately assured her that her embryos were safe but confirmed her suspicion: The clinic was closing because of the storm, and Kirsti wouldn’t be able to go through with the transfer the following day. In fact, they would have to start her cycle all over again. (Kirsti’s clinic did not respond to requests for comment.)
“It just felt like our earth was shattered,” she said. Five weeks of hormone injections had taken their toll on her body, both emotionally and physically. She had grown to dread the shots, which caused swelling in her buttocks, thighs, and stomach. “We had spent so much money, so much time. I was covered in bruises,” she said. “I hung up the phone and I just lost it. I lost it. I wasn’t even angry. I was just heartbroken.”
Aside from the sadness she felt over yet another hurdle in their fertility journey, Kirsti thought about all the money she and Justin had poured into the treatment, including borrowing from family. The $2,500 the couple had spent on fertility medications that month evaporated the moment Kirsti’s phone rang. If the couple were to restart the embryo transfer process, they would have to spend thousands more.
Because IVF is so costly, there is a large access gap between those who can afford the treatment and those who can’t. In a 2021 survey administered by researchers in Illinois who sought to better understand the demographics of IVF patients in the state, 75.5 percent of the respondents were white, 10.2 percent Asian, 7.3 percent Black, and 5.7 percent Latina.
Despite these hurdles, IVF is becoming increasingly popular. The treatment allows people to delay pregnancy for any number of reasons — to build a career, save money for a family, or find the right partner. And it’s a crucial tool for people struggling with infertility. In the U.S., that’s 1 in 5 women.
As IVF has grown more common, it has also become the target of political and legal attacks. In February, Alabama’s Supreme Court, dominated by conservative judges, ruled that embryos created in vitro should be thought of as children for the purposes of wrongful death lawsuits. The ruling had an immediate chilling effect on clinics throughout the state. A month later, Alabama lawmakers extended criminal and civil immunity protections to IVF clinics for their day-to-day operations. Manufacturers of products used in the course of IVF treatment get some immunity protections under the new law, too. But the law still leaves providers at risk because it doesn’t challenge the court’s assertion that embryos are people.
A billboard sponsored by the the Democratic National Committee as seen in February in Miami. The group sponsored 40 billboards across seven battleground states calling out the IVF ruling in Alabama. John Parra / Getty Images for DNC
This decision also has possible implications for doctors practicing IVF when a disaster hits, said Ulrich. “If you had an incubator on a power grid that failed, and you didn't have a backup or the backup failed — those embryos would have been lost,” said Ulrich. Perhaps patients would see the loss as an unavoidable accident — or perhaps they’d sue for wrongful death, she said. “It’s another reason to be careful.”
In the days after Hurricane Ian made landfall, Kirsti spent her time worrying about her family, her neighborhood, her house, and the animals at the zoo. Beneath it all, she felt a deep sense of despair. “I felt like every single piece of me was being hit and like every single thing I had was being ripped to shreds,” she said. But there was no doubt in her mind that she and Justin would try again.
For months, Kirsti’s embryos stayed safely frozen while she and a few other women she knew from the clinic waited to have their transfers rescheduled. The hurricane’s disruption meant their appointments would come after others already on the books, so she wouldn’t be penciled in until December, delaying her procedure even longer. The clinic agreed to waive the fees for the postponed transfer, but Kirsti and Justin still had to pay out of pocket for the costly medications.
On Halloween, she once again started preparing her body to carry a baby, taking a slew of medications and undergoing daily hormone injections. On the first of December, she completed the long-awaited transfer. Two weeks later, her doctors confirmed what she already knew based on a home test: Kirsti was pregnant. “I was over the moon,” she said.
She was also nervous: “We had been pregnant before and it always ended in loss.” As she and her husband put together the baby’s zoo-themed room they felt hopeful — but nothing was certain until August 8, 2023, when she gave birth to a healthy baby girl named Gracie.
A rainbow onesie and ultrasound pictures of the Mahons' daughter Gracie from April 2023. Courtesy of Kirsti Mahon
That day, the Naples coast was hot and sunny. As they looked down at their newborn daughter, Kirsti and Justin reflected on all it took to get there, after nearly four years of trying to start their family. “She was here and in our arms, and we just had this moment,” she said. “It was like, ‘We did it.’”
A few weeks later, Florida was hit by another Category 4 hurricane.
Roger Casupang was working in a coastal clinic on the north side of Papua New Guinea, an island nation of 9 million in the southwestern Pacific Ocean, when a pregnant woman burst into his facility. She was in labor, moments away from delivering twins. She also had a severe case of malaria, a life-threatening mosquito-borne illness common in tropical countries.
Casupang, an obstetrician, quickly took stock of the situation. When the parent is healthy, a twin pregnancy is twice as risky as a single pregnancy. Meanwhile, severe malaria kills nearly half of the people who develop it during pregnancy. The woman was exhausted and delirious. Because many of his patients walked for days to get medical care for standard ailments, Casupang didn’t know which province she had come from or how long she had been traveling before she reached his clinic.
What he did know was that the woman had arrived just in time. “She was actually pushing when she came in,” he said.
Casupang, who was born in one of Papua New Guinea’s highland provinces and had been practicing medicine on the island for the better part of a decade at the time, had seen pregnant women die in less dire circumstances. Against all odds, with limited medical resources and medicines at their disposal, Casupang and the other medical professionals at the clinic were able to deliver the twins safely. Both babies weighed less than three pounds each, a consequence of their mother’s raging infection. The twins were moved to the nursery while Casupang and his fellow physicians worked to stabilize the mother. She was reunited with her babies after 10 days of intensive care. “If this case had presented in a remote facility,” Casupang said, “the narrative would have been very different.”
Casupang’s patient was lucky to survive — but she also benefited from geography. On the coast, doctors see lots of patients with malaria, and many of those patients carry antibodies that protect them from severe infection.
But malaria is on the move.
A woman sleeps with her baby in the maternity ward of a hospital in Goroka in the Eastern Highlands Province of Papua New Guinea in 2009. Jason South / Fairfax Media via Getty Images
Temperatures are rising around the world but particularly in countries where the disease is already present. That warming coaxes mosquitoes toward higher elevations, even as temperatures have historically been too cold for the insects to thrive. In these high-altitude areas, mosquitoes are feeding on people who have never had malaria before — and who are much more susceptible to deadly infections.
“When malaria hits new populations that are naive, you tend to get these explosive epidemics that are severe because people don’t have any existing immunity,” said Sadie Ryan, an associate professor of medical geography at the University of Florida.
Pregnant people living in highland regions who have never had malaria before are worst-positioned to survive the bite of an infected mosquito. The very act of becoming pregnant creates a potentially deadly vulnerability to malaria. The placenta, the new organ that forms to nourish the fetus, presents new receptors for the disease to bind to.
Amelia K. Bates / Grist
Pregnant women are three times more likely to develop severe malaria compared to nonpregnant women. For people who can become pregnant, the climate-driven upward movement of malaria mosquitoes poses nothing less than an existential threat.
“In Western countries, especially where malaria is not endemic, there is this perception that malaria has been around for so long that we already know how to deal with it,” said Deekshita Ramanarayanan, who works on maternal health at the nonpartisan research organization the Wilson Center.
But that was never the case, and the perception is especially flawed now, as climate change threatens to rewrite the malaria-control playbook. “Pregnant people are hit with this double risk factor of climate change and the risks of contracting malaria during pregnancy,” Ramanarayanan said.
Hundreds of millions of people get malaria every year, and an estimated 2.7 million die from it, mostly in tropical and subtropical regions. In 2022, 94 percent of global malaria cases occurred in sub-Saharan Africa. High rates of the disease are also found in Central America and the Caribbean, South America, Southeast Asia, and the western Pacific. Papua New Guinea registered over 400,000 new cases in 2022. That same year the country accounted for 90 percent of the malaria cases in the western Pacific.
Malaria is carried by dozens of species of Anopheles mosquitoes, also known as marsh or nail mosquitoes. Anopheles mosquitoes carry a parasite called Plasmodium — the single-cell genus that causes malaria in birds, reptiles, and mammals like humans.
When the bite of an Anopheles mosquito introduces Plasmodium into the human bloodstream, the parasites travel to the liver, where they lurk undetectably and mature for a period ranging from weeks to a year. Once the parasites reach maturity, they venture out into the bloodstream and infect red blood cells. The host often experiences symptoms at this stage of the infection — fever, chills, nausea, and general, flu-like discomfort.
The earlier a malaria infection is caught, the better the chances that antimalarial medications can help prevent the development of severe malaria, when the disease spreads to critical organs in the body.
Pregnancy primes the body for infection.
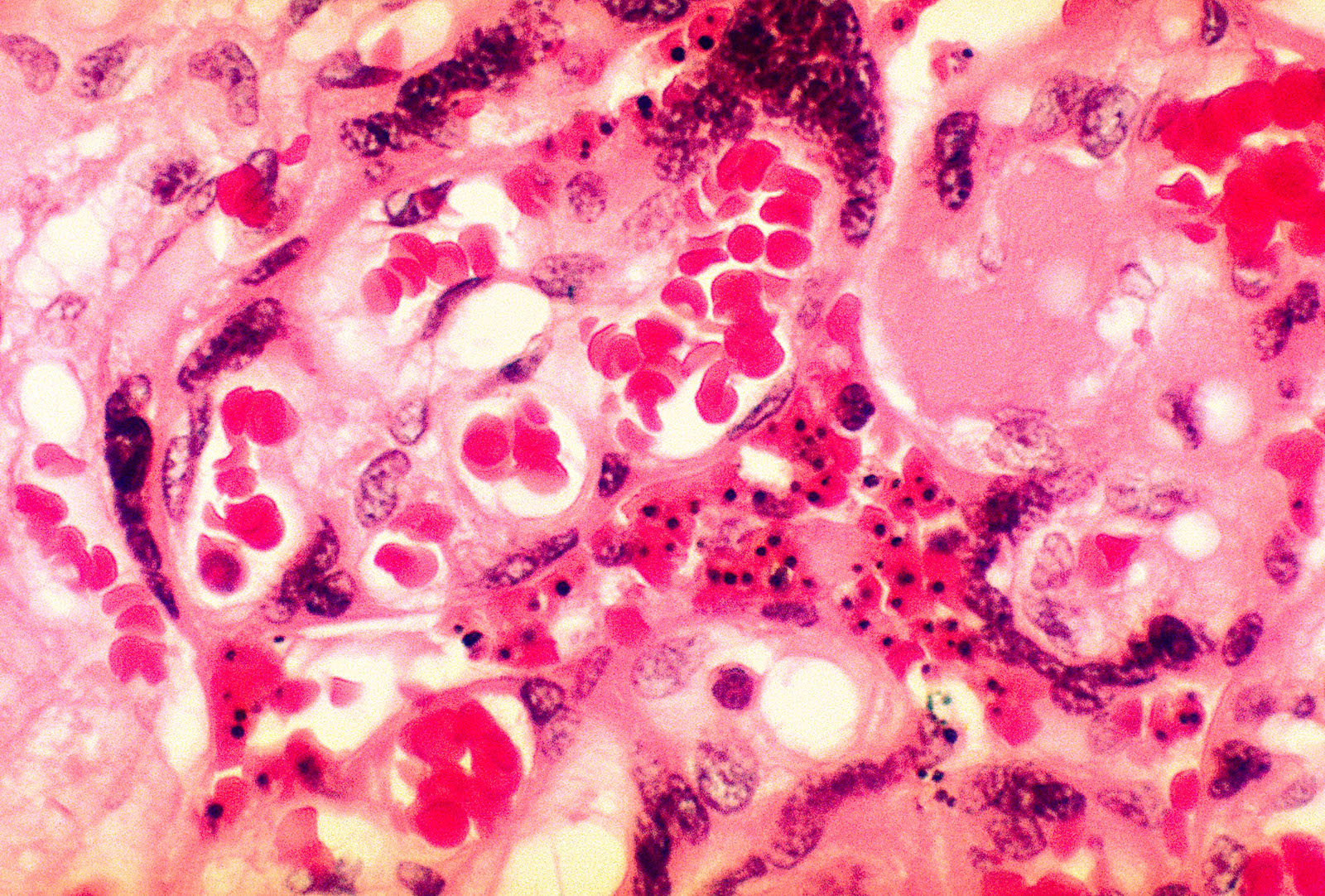
A photomicrograph of placental tissue revealing the presence of the malarial parasite Plasmodium falciparum. BSIP / UIG Via Getty Images
The immune system, when it is functioning properly, engages an arsenal of weapons to ward off bacteria, viruses, and other pathogens. But pregnancy acts like an immunosuppressant, telling the defense system to stand down in order to ensure the body does not inadvertently reject the growing baby. “Your immune system is, on purpose, dialed back so that you can tolerate the fact that you have this fetus inside of you,” said Marya Zlatnik, an obstetrician and gynecologist at University of California, San Francisco Medical Center.
Then there’s the added strain of supplying the baby with enough nutrients, vitamins, and minerals. The body must work overtime to provide for the metabolic needs of two. This factor, exacerbated by poverty, malnutrition, and subpar medical infrastructure in countries where malaria is commonly found, poses enormous challenges to maternal and fetal health. A malaria infection on top of those existing vulnerabilities introduces another, even more challenging set of obstacles.
The disease can produce severe maternal anemia, iron deficiency, or it can spread to the kidneys and the lungs and cause a condition known as blackwater fever. The disorder makes patients jaundiced, feverish, and dangerously low on vitamins crucial for a healthy pregnancy.
A woman with her newborn baby in the birthing suite at a hospital in Goroka in 2009. Jason South / Fairfax Media via Getty Images
Plasmodium parasites have spikes on them, similar to the now-infamous coronavirus spike proteins, that make them sticky and prone to clogging up organs. If Plasmodium travel to the placenta, the parasites bind to placental receptors and cause portions of the placenta to die off. “It changes the architecture of the placenta and the ways nutrients and oxygen are exchanged with the fetus,” said Courtney Murdock, an associate professor at Cornell University’s department of entomology. The placental clots interfere with fetal growth, and they’re one of the reasons why a pregnant woman is between three and four times more likely to miscarry if she has a malaria infection, and why babies born to mothers sick with malaria come out of the womb malnourished and underweight.
“You see the placenta start to fail,” Casupang said. Fetal mortality is closely tied to how much of the placenta becomes oxygen deprived. “The babies come out with very low birth weights,” he said. If the placental clots are extensive, “they usually die.”
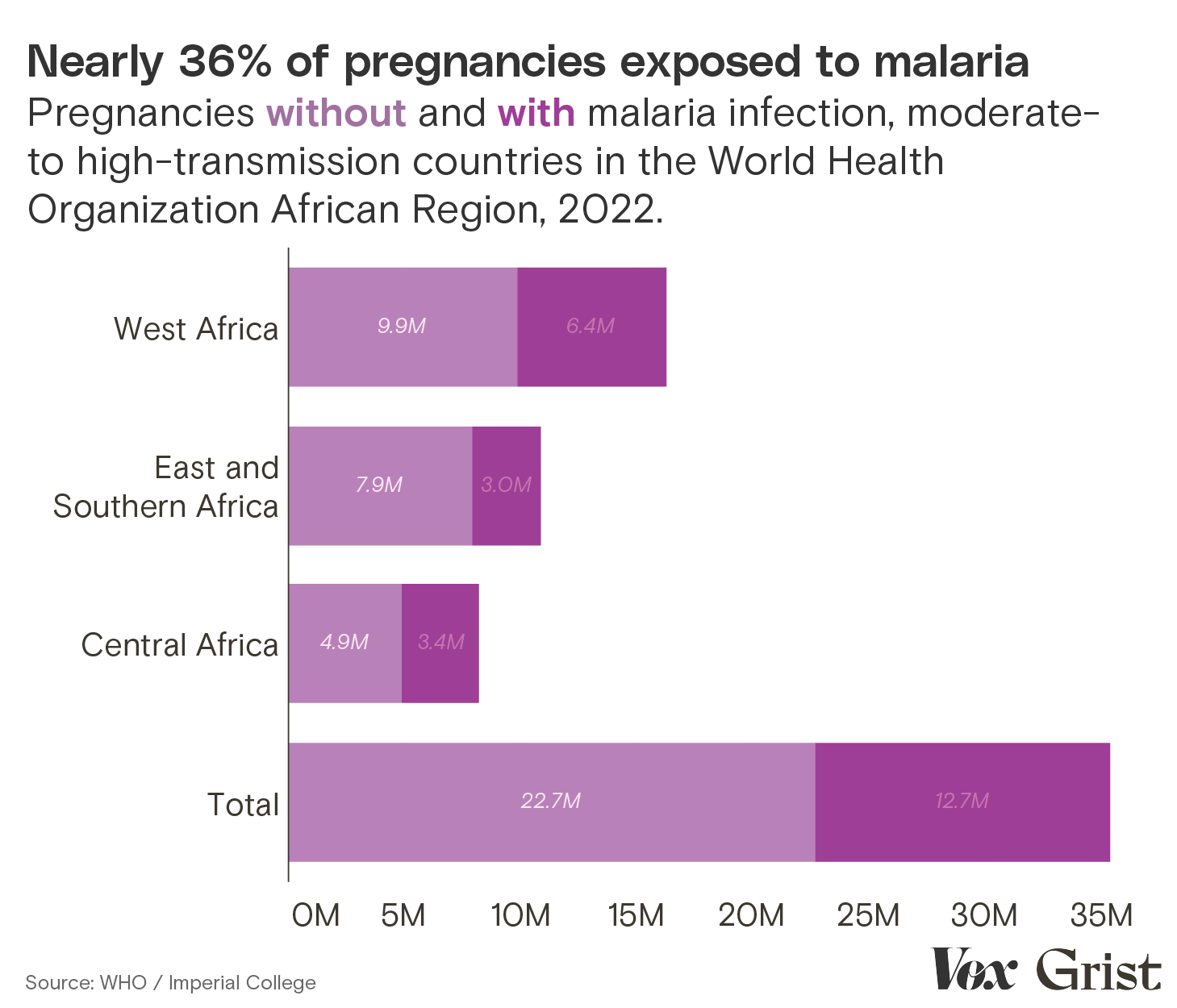
In 2020, approximately 122 million pregnancies — about half of all pregnancies worldwide that year — occurred in areas where people were at risk of contracting malaria. A 2023 study estimated that 16 million of these pregnancies ended in miscarriage, and 1.4 million in stillbirth.
Researchers don’t know exactly how many of those miscarriages and stillbirths occurred in individuals who were bitten by malaria-infected mosquitoes.
Researchers have said that out of all the high-impact infectious diseases — including Ebola, mpox (formerly known as monkeypox), and MERS — malaria is the “most sensitive to the relationship of human populations to their environment.” In Papua New Guinea, the coastal zones that sit near or at sea level have long had environmental conditions that foster the development and spread of the Anopheles mosquito. Cases of malaria topped 1.5 million in 2020, and the vast majority occurred in the nation’s lowlands.
At 4,000 feet or more above sea level, where some 40 percent of the Papua New Guinean population lives, temperatures have historically been too cold for Anopheles mosquitoes to thrive year-round. There have been seasonal outbreaks of malaria in those zones, but the background hum of malaria present in the lowlands largely disappears above the 4,000 feet mark. At 5,200 feet above sea level, periodic freezes kill mosquitoes and prevent them from establishing widely, making malaria infections there very rare.
But climate change is expanding the areas where Anopheles mosquitoes and the Plasmodium they carry flourish by fostering warmer, wetter environments. Mosquitoes thrive in the aftermath of big storms, when the insects have ample opportunity to breed in standing pools of water.
At the same time, higher-than-average temperatures almost everywhere in the world mark the beginning of a new chapter in humanity’s long struggle to contain mosquitoes and the diseases they carry. Anopheles mosquitoes grow into adults more quickly in warmer weather, and longer warm seasons allow them to breed faster and stay active longer.
This poses problems in areas where Anopheles mosquitoes are already prevalent, and in regions the insects are poised to infiltrate. The mountainous regions of the world — the Himalayas, the Andes, the East African highlands — are thawing as average global temperatures climb. What used to be an inhospitable habitat is becoming fertile ground for malaria transmission.
Women pick strawberries in a highland field in Enga Province, Papua New Guinea, in December 2019. Betsy Joles / Getty Images
Piglets stand on the road near Kapandas village in the highlands of Papua New Guinea in December 2019. Betsy Joles / Getty Images
Like their mosquito hosts, Plasmodium parasites are sensitive to temperature. The two most common strains, Plasmodium falciparum and Plasmodium vivax, like temperatures in the range of 56 to 95 degrees Fahrenheit. The warmer the weather, the more quickly the parasites are able to reach their infectious stage. A study that examined temperatures suitable to Plasmodium in the western Himalaya mountains predicted that, by 2040, the mountain range’s high-elevation sites — 8,500 feet above sea level — “will have a temperature range conducive for malaria transmission.”
There’s little data on the rate at which Anopheles mosquitoes and the parasites they carry are moving upward in Papua New Guinea, but research shows temperatures across Papua New Guinea were, on average, just under 1 degree Celsius (1.8 degrees F) warmer between 2000 and 2017 than they were a century prior. A report conducted by the World Bank Group noted that this temperature rise “has been fastest in the minimum temperatures,” meaning climate change jeopardizes the overnight low temperatures that are so essential to mosquito control. Anecdotally, doctors and nurses working in the country’s colder regions say they have seen a familiar pattern begin to change.
Stella Silihtau works in the emergency department at the Eastern Highlands Provincial Health Authority in Goroka, a town of 20,000 that sits at 5,200 feet above sea level on a major road that connects the scattered highland cities and towns to the communities along the coast. Silihtau and her colleagues are no strangers to malaria. Hundreds of people in Goroka and surrounding highland towns grow cash crops like coffee, tea, rubber, and sugarcane and ferry them down to the coast every week to sell to plantations and community boards. The highland dwellers are bitten by mosquitoes at lower elevations, and end up at the hospital where Silihtau works weeks later, sick with malaria. Over the past year, she’s seen unusual cases starting to crop up.
“We’ve been seeing a lot of patients that are coming in with malaria,” said Silihtau, who grew up in the lowlands. Many of these cases have been in people who have not traveled at all. “We’ve seen mild cases, severe cases, they go into psychosis,” she said.
A fire set to repel mosquitoes in Milne Bay Province, Papua New Guinea. Eric Lafforgue / Art in All of Us / Corbis via Getty Images
Silihtau and her colleagues don’t have the time or staff to keep close track of how many locally acquired malaria cases have been treated at the hospital over the past year. But Silihtau estimates that when she first started working at the hospital in Goroka two years ago, she saw one case per eight-hour shift, or none at all. Now, she sees between two and three cases of malaria per shift, some of them in individuals who have not traveled outside the boundaries of Papua New Guinea’s highland zones. “It’s a new trend,” Silihtau said.
The new dangers that the upward movement of malaria mosquitoes pose to pregnant people are obfuscated by positive signals in malaria cases globally.
Global malaria deaths plummeted 36 percent between 2010 and 2020, the dive driven by wider implementation of the standard, relatively low-cost treatments that research shows are incredibly effective at preventing severe infections: insecticide-treated mosquito nets, antimalarial drugs, and malaria tests.
This promising trend stalled in 2022, when there were an estimated 249 million cases of malaria globally — up 5 million from 2021. Much of the increase can be attributed to the COVID-19 pandemic, which slowed various global infectious disease control efforts as health care systems tried to contain an entirely new threat. Funding for malaria control is also falling short. Countries spent a total of $4.1 billion on malaria in 2022, nowhere near the $7.8 billion in funding the World Health Organization says is necessary annually to reduce the global health burden of the disease 90 percent by 2030.
Meanwhile, cases have been rising in step with the spread of a mosquito called Anopheles stephensi, a species that can carry two different strains of Plasmodium and, unlike the rest of its Anopheles brethren, thrives in urban environments. Efforts to control malaria in both urban and rural settings are stymied by the quickening pace and severity of extreme weather events, which scramble vaccination and mosquito net distribution campaigns, shutter health clinics, and interrupt medical supply chains. Record-breaking storms, which destroy homes and public infrastructure and create thousands of internal migrants, force governments in developing countries to choose where to allocate limited funding. Infectious disease control programs are often the first to go.
The world’s slowly warming highland regions are one small thread in the web of factors influencing the prevalence of malaria. But because of the lack of immunity among populations in upper elevations, the movement of malaria into these zones poses a unique threat to pregnant people — one that may grow to constitute a disproportionate fraction of the overall impact of malaria as climate change continues to worsen.
“Pregnant women are going to be a high-risk population in highland areas,” said Chandy C. John, a professor and researcher at Indiana University School of Medicine who has conducted malaria research in Kenya and Uganda for 20 years. John and his colleagues are in the process of analyzing their two decades of health data to try to tease out the potential effects of climate on malaria cases. “What are we seeing in terms of rainfall and temperature and how they relate to risk of malaria over time in these areas?” he asked. His study will add to the small but growing body of research on how temperature shifts in high elevations contribute to the prevalence of malaria.
Controlling and even eradicating malaria isn’t just possible; it has already been done. Dozens of countries have banished the disease; Cabo Verde recently became the third African country to be certified as malaria-free. “Malaria is such a complex disease,” said Jennifer Gardy, deputy director for malaria surveillance, data, and epidemiology at the Bill and Melinda Gates Foundation, “but that complexity is kind of beautiful because it means we’ve got so many different intervention points.”
In addition to the typical interventions such as mosquito nets, the Papua New Guinea National Department of Health has had some success with medical therapies for people who develop malaria infections while pregnant. Doctors there and in many other malaria-endemic places use intermittent preventive treatment on pregnant women. The antimalarial is administered orally as soon as patients learn they are pregnant and, if taken on regularly, can significantly reduce the chances of severe malaria over the course of gestation. The treatment remains difficult to access in highland regions, as malaria has historically been uncommon there. If governments and hospitals pay attention and get these medicines into places where rising temperatures are changing climatic constraints on mosquitoes, they will save lives.
A mother feeds her newborn baby in the maternity ward of a hospital in Goroka in 2009. Jason South / Fairfax Media via Getty Images
The smartest solutions are those that address malaria as a symptom of a wider system of inequity. Papua New Guinea is a “patriarchal society where men get the best treatment,” Casupang, who now works for an international emergency medicine and security company called International SOS, said. “Women are pretty much regarded as commodities.” Most married women must seek permission from their husbands to seek medical care at a facility, and permission is not always granted. Many women are also prevented from seeking medical attention by poverty, by the quality of the roads that connect rural villages to cities, and because they don’t recognize the symptoms of malaria or understand the risks the infection poses to themselves and their unborn children, Casupang said. Just 55 percent of women in Papua New Guinea give birth in a health facility, a partial function of the fact that the country currently has less than a quarter of the medical personnel it needs to care for mothers, babies, and children.
“There are quite a number of factors that will determine the outcome of a mother that has malaria,” Casupang said. “The most important thing is access to a health care facility.” He’s one of many experts who argue that better infrastructure, improvements in education, and the implementation of policies that protect women and girls double as malaria control measures — not just in Papua New Guinea but everywhere poverty creates footholds for infectious diseases to take root and flourish.
“Education, a living wage, sanitation, and all of these other very basic things can do so much for a disease like malaria,” John said. “It’s not a mosquito net or a vaccine, but it can make such a huge difference for the population.”
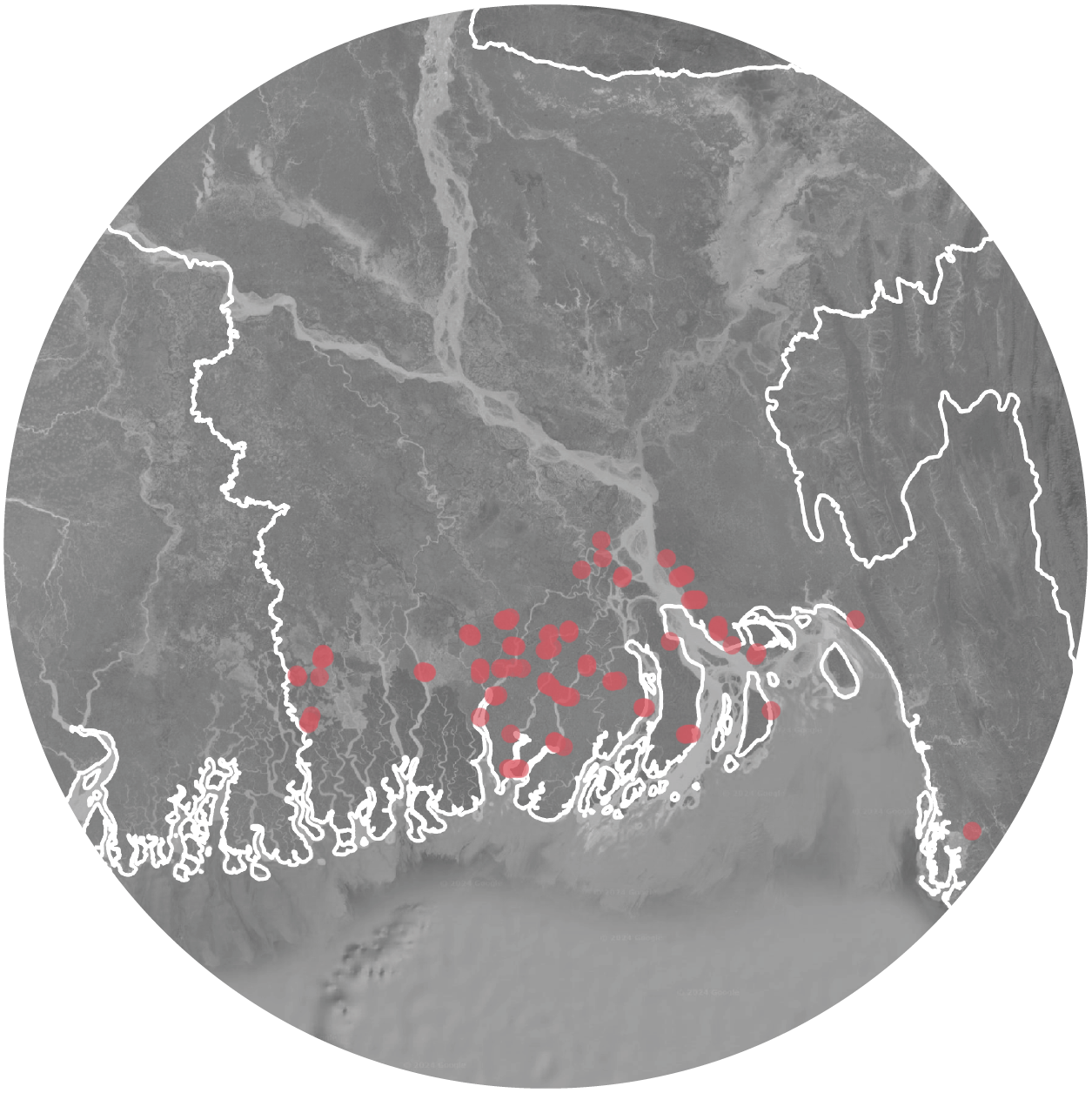
Today, 30-year-old garment factory worker Khadiza Akhter lives in Savar, a suburb of Dhaka, the capital of Bangladesh. Her small concrete house is clean and organized. Green shutters frame the windows, and clothes hang on lines outside her front door. A water spigot sticks out of the concrete next to the drying laundry, and the turn of a white plastic knob is all it takes for clear, clean water to rush out. Akhter calls it “a blessing of God.”
Akhter grew up some 180 miles south of Savar, in Satkhira — a district home to 2.2 million people on a river delta where, in recent decades, fresh water has become scarce. As sea levels rise, rivers dry up, and cyclones become more severe, Satkhira and the other low-lying districts that surround it have been among the first in the world to experience the sting of climate change-driven saltwater intrusion — the creep of seawater inland.
The memory of drinking water tainted with salt is burned into Akhter’s mind. “It felt like swallowing needles,” she told Grist and Vox in Bengali. “It doesn’t quench your thirst.” The water was so salty Akhter couldn’t properly clean herself with it. The sodium in the water prevented soap from forming bubbles and left powdery streaks on her skin as it dried. Her hair fell out, and she itched all over.
When she hit puberty, she had to wash her cloth menstrual pads in salty water. The monthly exposure to salt in her pads made her break out in sores. Akhter’s menstrual cycle became erratic. “One month, it showed up unexpectedly early, catching me completely off guard,” she said. “The next month, it seemed to disappear altogether.” She sought medical advice at the Shyamnagar Upazila Health Complex, the local hospital in Satkhira, but there was no long-term fix available to her, beyond stopping her period altogether with hormonal birth control pills. She left Satkhira a decade ago, when she was a teenager, and moved to Savar, known for having some of the cleanest water in Bangladesh.
Khadiza Akhter fills up pitchers with water from a spigot in front of her home in Savar, Bangladesh. Mahadi Al Hasnat
When Akhter first arrived in Savar, she had trouble adapting to city life. She wasn’t used to eating food cooked on a gas stove, and went to extreme lengths to avoid it. “I used to buy biscuits or cakes from the office canteen and sometimes starved,” she said. But, Akhter, who knew she wanted children someday, pushed through. “All I ever wanted was a better life for my kids — a life where they wouldn’t have to worry about food or clean water,” she said.
Studies have shown that saltwater consumption has negative, long-lasting effects on nearly every stage of a woman’s reproductive cycle, from menstruation to birth. Akhter knew that if she stayed in Satkhira and started a family of her own there, she’d be putting herself in real danger. She’s not the only person in her region to leave in search of cleaner water. Millions of Bangladeshis have been internally displaced by flooding in the past decade, and experts say saltwater intrusion is one of the factors driving migration from rural regions of Bangladesh to urban centers.
In some ways, Akhter is one of the lucky ones. She got out of Satkhira before saltwater consumption led to high blood pressure, a hysterectomy, or worse. But the women, and other people with uteruses, who remain in Satkhira are suffering from reproductive health effects — issues that could become common elsewhere in the coming years. As sea levels rise and intensifying storms stress infrastructure systems along coasts around the world, salt water threatens to infiltrate freshwater drinking supplies in countries like Egypt, Italy, the United States, and Vietnam. The issue, a 2021 study stated, “has become one of the main threats to the safety of freshwater supply in coastal zones.” The health of women living in these areas is on the line.
Jahangirnagar University, a campus in Savar where Akhter and her family often spend their time. Mahadi Al Hasnat
Southwestern Bangladesh is accustomed to encroaching salt water. The region sits adjacent to where the Padma River — known as the Ganges in India — empties into the Bay of Bengal. Most of the Bangladesh delta is less than 2 meters, or 6.5 feet, above sea level, with some areas at or even below the tide line. When cyclones wheel into the bay, storm surge pushes salt water inland, flooding the area.
For generations, communities in Satkhira adapted to the ebb and flow that defines the delta ecosystem. In the late 1960s, when a catastrophic period of cyclone-driven storm surge submerged rice paddies in salt water and ruined livelihoods, Satkhira was one of the first districts in Bangladesh to turn those paddies into shrimp farms. Small-scale farmers took advantage of storm surge — trapping seawater in ponds and paddies to cultivate shellfish — and paved the way for other parts of coastal Bangladesh to do the same. Today, shellfish farms have expanded into roughly 675 square miles of land, most of it in southern Bangladesh. Annual shellfish exports are valued in the hundreds of millions of U.S. dollars, and the industry employs more than a million people directly, and millions more indirectly.
But the district’s legacy of hard-fought resilience is being undone by climate change.
Savar, Bangladesh. Mahadi Al Hasnat
Already, sea level rise has pushed the saline front more than 62 miles inland along the country’s 450-mile coastline. Climate models indicate that a 380-square-mile area in coastal Bangladesh, home to 860,000 people, could be under the high tide line by the end of this century. Every millimeter of sea level rise contributes to more expansive and intense saltwater intrusion in soil and freshwater resources.
Fishermen work in a marsh a few hundred feet from where Akhter lives in Savar. Mahadi Al Hasnat
The trend is made worse by the region’s growing shrimp and prawn industry. Black tiger shrimp, the main species of shrimp farmed in Bangladesh, thrive in brackish water — water that is saline but not quite as salty as seawater. When Satkhira began to embrace aquaculture and shrimp farming, the government neglected to study the potential risks of adding saline to freshwater ponds in order to make them suitable for shrimp farming. Over time, salt from the shrimp fields leached into ponds and other in-ground freshwater containers, further contaminating limited drinking water supplies. A 2019 report that tested salinity in 57 freshwater ponds in Satkhira found that 41 of them contained water that was too salty for drinking.
The Padma River, which carries fresh water from Nepal through India to Bangladesh, is another source of salinity. The river supplies much of the fresh water Bangladeshis use for irrigation, farming, freshwater fishing, and drinking. But the Padma’s flow into Bangladesh is restricted seasonally by India, which controls a dam in West Bengal called the Farakka Barrage. During dry periods, the flow of water coming into Bangladesh from India slows and the volume of river water going into the ocean weakens, allowing seawater to work its way up the Padma. When heavy rain falls, the river swells and salt water is pushed back out, expunging the river of its salinity and transforming the river back into a freshwater resource.
“The people are trapped,” said Zion Bodrud-Doza, a researcher at the University of Guelph in Canada who studies saltwater intrusion in Bangladesh. “When you don’t have water to drink, how do you live?”
In 2008, Aneire Khan, a researcher at Imperial College London, visited Dacope, a division of the Khulna district, which borders Satkhira in southwest Bangladesh. She met a gynecologist there who told her that an unusual number of pregnant women were coming to him with gestational hypertension and preeclampsia.
The former is defined as two separate blood pressure readings of greater than 140 over 90 in the second half of the pregnancy. The latter occurs when those high blood pressure readings are accompanied by high levels of protein in the urine.
Both conditions affect how the placenta develops and embeds into the uterine wall, said Tracy Caroline Bank, a maternal fetal medicine fellow physician at The Ohio State University Wexner Medical Center. Patients with either condition “have a higher risk of things like a preterm delivery, of fetal loss,” she said, in addition to “a higher risk of the baby growing too small.” Premature babies are dealt a bad hand before they take their first breaths: Low birth weights are linked to poor development, cognitive impairments, cerebral palsy, and psychological disorders.
The gynecologist Khan spoke to said that high blood pressure readings, especially in women, were occurring with more frequency. Other medical professionals Khan spoke to in Khulna confirmed that observation. They thought salt water may be the culprit.
Amelia K. Bates / Grist
People who drink water with small amounts of salt in it can grow acclimated to moderate salinity over time. Khan, who was traveling between London and Bangladesh at the time, tasted the water in Khulna and was surprised to encounter immediate, undeniable salinity. It was “very, very salty,” she said. She conducted a survey of blood pressure levels in pregnant women living along the coast and compared the data to blood pressure in women living inland. More than 20 percent of the women living in coastal zones had been diagnosed with a hypertensive disorder, compared to less than 3 percent of women living in Dhaka. It was clear that a serious public health threat was growing along the coast, but no formal epidemiological study of saltwater intrusion and reproductive health in Bangladesh existed at the time. Khan set out to change that.
In 2011, three years after she spoke to the gynecologist in Khulna — the man who became her co-author — Khan published a study that showed that hypertension, or high blood pressure, in Dacope occurred seasonally. Out of the 969 pregnant women they analyzed, 90 presented with hypertension. In the wet monsoon months, heavy rains filled ponds with fresh water and diluted salt concentrations in rivers. During the dry season, lack of rainfall caused people to turn to other sources of drinking water that became steadily saltier over the course of the season. Of the 90 cases of gestational hypertension that Khan documented, 70 occurred during the months of November and April, the periods with the least amount of rainfall.
The World Health Organization recommends that adults consume no more than 5 grams of salt per day, about a teaspoon worth. Khan ultimately discovered that women in Dacope were getting more than three times that amount per day from their drinking water alone during the dry months.
Consumption isn’t the only way that salt water endangers women’s reproductive health. As Akhter learned as an adolescent, using salt water to wash cloth menstrual pads presents additional dangers. The water “doesn’t clean well,” said Mashura Shammi, a professor at Jahangirnagar University in Bangladesh who studies saltwater intrusion and the effects of pollutants on health. “The salt makes the cloth very hard,” she added, and can cause scratches in the vagina that lead to infection.
Other women in southwestern Bangladesh, particularly those who make a living working in shrimp aquaculture or fishing in the rivers, suffer even more intense health repercussions. Standing in salt water every day can produce chronic uterine infections and uterine cancer. The International Centre for Climate Change and Development, a research institute, interviewed women from Bangaldesh’s coastal zones and found anecdotal evidence of a host of saltwater-linked health outcomes. “I have cut off my uterus through surgery due to my severe infections,” one 32-year-old woman said. “And I am not the only one, there are many like me.” In the same report, a doctor from the Shyamnagar Upazila Health Complex said she had noticed “an increase in infertility, irregular periods, and pelvic inflammatory disease.” The doctor said that the majority of her female patients over the age of 40 have had hysterectomies or have undergone procedures to eliminate the lining of the uterus in order to lessen heavy menstrual bleeding.
Roughly 40 percent of the world’s population lives within 60 miles of a coast, and more than 100 countries are at risk of saltwater intrusion. By the end of 2019, 501 cities around the world had reported a saltwater intrusion crisis of some degree — more than a fifth of them home to more than 1 million people each. “Bangladesh isn’t the only country that’s going to be affected by salinity,” Khan said. “Vietnam, China, the Netherlands, Brazil — salinity in the coastal areas is going to be a huge issue, and is already a problem.”
Nearly every solution to saltwater intrusion hinges on trying to keep seawater out of fresh water to begin with. Armoring coastlines with sea walls, levies, sandbags, and other hard infrastructure is the first line of defense in many countries. Those with water and money to spare can artificially “recharge” underground freshwater aquifers to preserve the natural tension between fresh water and salt water. Governments can also put restrictions on how much water farmers can pull from underground resources.
Preventative measures are more effective than fixes put in place after the fact. It’s nearly impossible to clean salt out of fresh water without the aid of expensive and energy-intensive desalination equipment, which most countries do not have. A medium-size desalination plant, which is an incredibly energy-intensive piece of infrastructure, costs millions of dollars to build and then millions more in annual operation costs. Even in very rich nations, runaway saltwater intrusion poses risks to infrastructure and people. Most water supply networks’ intake stations in the U.S., for example, are not outfitted with desalination technology. Once saltwater intrusion reaches those stations, they have to be shut off to avoid pulling the water in.
The creep of seawater inland
While global salinity monitoring is spotty, evidence of saltwater intrusion continues to grow.
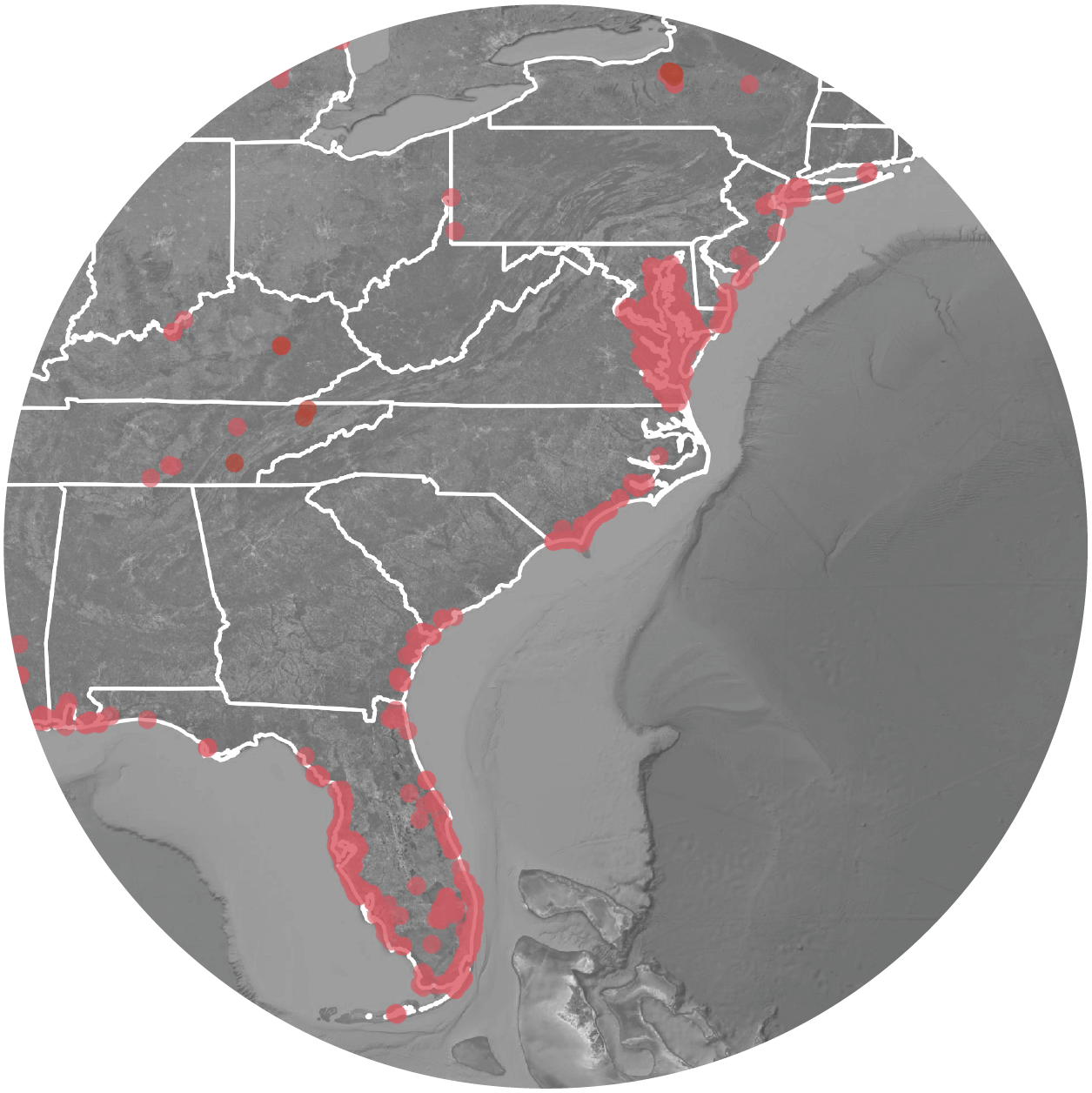
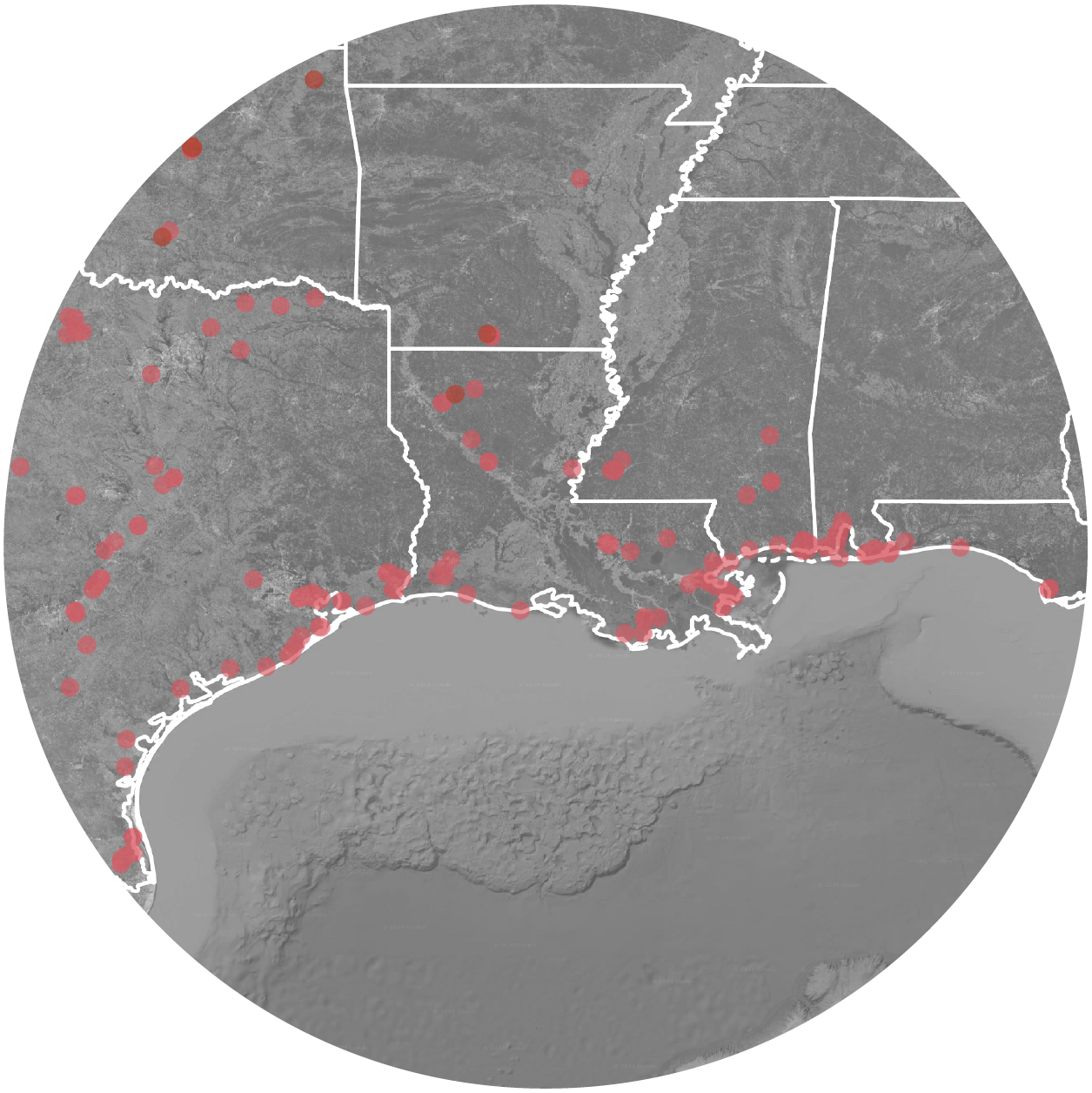
Last year, drought in the Mississippi and the Ohio River valleys weakened the flow of water in the Mississippi River, and a massive wedge of seawater from the Gulf of Mexico started to creep north. As the wedge moved upstream along the bottom of the river, intake stations in Plaquemines Parish, Louisiana, started sucking it in. More than 9,000 residents couldn’t drink water from their taps, and local officials started distributing bottled water. Rainwater eventually eased the drought and forced the wedge back toward the ocean. Water in Plaquemines Parish is currently safe to drink again, though experts warn salt water poses a long-term threat to drinking water in southeast Louisiana.
Saltwater intrusion “is an issue along most of the coastline in America,” said Chris Russoniello, a professor of geological sciences at the University of Rhode Island. California, Louisiana, New Jersey, New York, and Rhode Island are some of the states that are already confronting intrusion. But exactly how much of a threat it poses to communities “varies drastically from place to place,” Russoniello said. How much funding states direct to keeping saltwater intrusion at bay will determine the extent to which people feel the burden of intrusion. Many states already lack sufficient drinking water protections and infrastructure, particularly in low-income and minority areas. Saltwater intrusion is likely to exacerbate existing drinking water inequities. But, in general, the U.S. is much better equipped to address saltwater intrusion than other countries grappling with similar issues.
“If the water is saline, you cannot make it fresh water in the blink of an eye,” Bodrud-Doza said. “People are trying to survive, but people need to leave.” Coastal Bangladesh and southeast Louisiana have that, at least, in common. Sea level rise will force a substantial portion of the population in both places to migrate inland. In areas where the encroaching tide, deadly storm surge, and widespread saltwater intrusion are inevitable, there will eventually be no option but retreat. “It’s something we need to think about as a society,” Russionello said. For the women already living on the front lines of a crisis that robs them of their health, reproductive organs, and pregnancies, retreating from the coastline is no longer a question of if, but how.
Shamim, Muntaha, and Khadiza Akhter at home in Savar. Mahadi Al Hasnat
Akhter and her husband, Shamim, grew up in adjacent villages and met when they were children. They began dating in high school and later indicated to their families that they wanted to be married. Akhter was living in Savar when her marriage to Shamim was arranged by her parents. After they were married in a traditional ceremony in Satkhira, Akhter temporarily moved to Shamim’s village, where the salt levels in the drinking water were even higher than they had been in her home village. The couple tried purifying the water with aluminum sulfate powder and boiling the water with herbs. As a last resort, Shamim installed a water filter he obtained in Dhaka. Nothing helped.
Akhter permanently relocated to Savar with Shamim, and, soon after, became pregnant and gave birth to her first daughter, Miftaul. Two years later, she gave birth to a second healthy girl, Muntaha. At first, the family lived together in Savar. But Akhter and Shamim both work full time, and they couldn’t afford day care for both children. Their older daughter, Miftaul, who is now 5, lives in Satkhira with her grandparents for most of the year, and Akhter worries about the impact that saltwater intrusion will have on her young daughter’s life.
Akhter’s younger daughter, Muntaha, looks out a window. Mahadi Al Hasnat
“It’s not ideal for her health, especially now that she’s growing,” Akhter said. “She already has trouble showering with salty water.” Miftaul has begun attending school in Satkhira, but Akhter and Shamim plan to bring her back to the city, where the schools and water quality are better, as soon as possible.
Akhter doesn’t want her children to relive a version of her own difficult childhood. A piece of her heart will always live in Satkhira, she said, but her future, and her daughters’ futures, are anchored in Savar. “I don’t want them to go through the struggles we faced.”
When Rupa Basu was pregnant with her second child, her body temperature felt out of control — particularly as her third trimester began in the summer of 2007. It wasn’t particularly hot in Oakland, California, with high temperatures reaching 80 degrees Fahrenheit. Still, she felt uncomfortably warm even as her colleagues and friends were unbothered.
As her October due date approached, she drank extra fluids and avoided going outside during the hottest stretch of the day. “This is really weird,” she recalls thinking. She wondered if there could be a biological mechanism at work.
That notion had troubling implications. “If this is a biological response, imagine what’s happening in places like India and Africa where the heat can get to an unbearable 130 degrees Fahrenheit,” Basu remembers thinking. As a researcher at the California Environmental Protection Agency’s Office of Environmental Health Hazard Assessment, Basu knew that other vulnerable populations, notably the elderly, were particularly susceptible to heat.
But she couldn’t find any answers to one fundamental question: do higher temperatures lead to premature births or other pregnancy complications?
Rupa Basu poses for a photo while pregnant with her second child in June 2007.
Courtesy of Rupa Basu
As Basu prepared for her second baby’s delivery, she began gathering state weather data and birth records to identify preterm births, those that occur prior to 37 weeks of gestation. Preterm birth is linked to a wide variety of health conditions, including anemia, respiratory distress, jaundice, sepsis, and retinopathy — and, at worst, infant mortality.
Researchers, including Basu, had already documented the impacts of air pollution on adverse pregnancy outcomes. But heat was, at the time, uncharted terrain — and the suggestion that it might have an effect was met with skepticism. Colleagues, particularly those who had not ever been pregnant, implied she was wasting her time. But when Basu published her study, her findings spurred similar research all over the world.
Basu analyzed 60,000 summertime births — those taking place between May and September — from 1999 to 2006, across 16 California counties. She found higher rates of preterm births during higher temperatures. She published the research in 2010, and even though she focused on California, it was the first large-scale epidemiological study looking at preterm delivery and temperature conducted anywhere in the world.
What was especially shocking, Basu said, was how much greater the risk was for Black mothers — 2.5 times higher than for white populations.
“How did we miss this for so long?” Basu asked. “Women are often the last to get studied. But the most vulnerable people are those who are pregnant.”
Those vulnerabilities are intensifying. In the last year, the hottest on record, 6.3 billion people — notably in South and East Asia and the African Sahel — experienced at least 31 days of extreme heat, hotter than 90 percent of documented temperatures between 1991 and 2020, according to a new report.
Breast milk is fed via tubes to a preterm infant at a neonatal intensive care unit in Washington, D.C., in 2017. Astrid Riecken / The Washington Post via Getty Images
As human-caused climate change continues, the number, intensity and duration of heat waves will only get worse. Without intervention, those heat waves will cause millions of babies around the world to be born preterm. Higher temperatures will also have knock-on impacts to gestational and fetal health. As temperatures rise, so does drought and air pollution, which also increases the risk of preterm birth or low birthweight babies. Pollutants from vehicle combustion, including nitrogen oxides and volatile organic compounds, react in sunlight to form ozone. And the U.S. Environmental Protection Agency calculated that extreme heat events will also lead to more wildfires, leading to air pollution that is expected to cause thousands of additional preterm births.
Basu began research on pregnant people because they are woefully understudied and they represent one of the most vulnerable populations. Now that there is strong evidence that heat exacerbates adverse birth outcomes, she hopes it will instigate policy change, promote awareness, and ultimately, decrease risk and disparities. “We need to take more action,” she said. “This is preventable.”
Emergency medical technicians respond to a pregnant woman suffering from dehydration in July 2023 in Eagle Pass, Texas. Brandon Bell / Getty Images
In the 14 years since Basu’s initial paper, dozens of studies have confirmed that higher temperatures and heat waves are linked to preterm birth as well as stillbirth.
In 2020, Basu co-authored a review of 57 studies that found a significant association between air pollution and heat exposure with preterm birth and low birth weight. Scientists have found an association between heat exposure and preterm birth rates in every developed nation, and in the few developing nations to conduct studies so far.
While it’s not yet clear how heat triggers preterm birth, there are several hypotheses — including dehydration, hormonal releases that rupture membranes surrounding the fetus, or poor blood flow between parent and unborn child.
This research has taken place against a backdrop of a worsening maternal health crisis in the U.S., particularly in marginalized communities. The U.S. has the highest rate of preterm births in the developed world. Kasey Rivas, associate director of strategic partnerships at the March of Dimes and a co-author of a recent report on birth outcomes and disparities, told me that maternal health disparities in the U.S. stem largely from systemic racism and are worsening due to climate change.
Amelia K. Bates / Grist
A 2023 study found that the average preterm birth rate was 7.9 percent across North America, Australia, New Zealand, and Europe in 2020; but the United States’ preterm birth rate was higher — 10 percent. By comparison, the highest population-wide preterm birth rate in the world is 13.2 percent in South Asia. U.S. rates of preterm birth increased 4 percent between 2020 and 2021 — and rates were far higher in Black women (14.8 percent) compared to white women (9.5 percent), according to the March of Dimes report. “The data were disturbing and disheartening,” Rivas said.
In 2023, a team of scientists decided to take a closer look at a notoriously deadly heat wave in Chicago in 1995 during which over 700 died as high humidity made 106 degrees feel like a hellish 120. “If we didn’t see a racial effect during this event, we won’t see it anywhere,” study co-author Joan Casey, an environmental epidemiologist at the University of Washington in Seattle, recently told me.
Casey and her colleagues found convincingly stark racial disparities. The mean monthly incidence of preterm birth rose 16.7 percent beyond what was expected for Black mothers six months after the heat wave. No such link was seen in non-Hispanic white births.
Further, a study conducted in Harris County, Texas, which includes Houston, the fourth largest U.S. city, found that the risk of preterm birth was 15 percent higher following extremely hot days — and had the greatest impact on communities of color that lived in neighborhoods with more concrete than trees.
Clayton Aldern / Grist
That finding points to the reasons behind the racial gap in preterm births linked to heat waves. Preterm birth has been linked to a number of factors including inadequate nutrition, exposure to air pollution, lack of access to quality health care, lack of air conditioning, or having a job working outdoors — or several of these at once. Heat only worsens existing risks.
And communities of color are more likely than white communities to face all of these risk factors, including heat. Predominantly Black neighborhoods were redlined, or deemed most risky, beginning in the 1930s when insurance companies created maps assigning investment risk levels based on race. Today, those redlined areas have more industrial facilities, excessive truck traffic, and a heavier pollution burden — and often, the least shade or green space. Areas dominated by concrete, asphalt, and buildings experience hotter temperatures due to the urban heat island effect, the phenomenon in which gray infrastructure absorbs and holds more heat than forests or waterways.
Fresno County, California, which has some of the worst air pollution in the United States, exemplifies this pattern. Venise Curry, a consultant for community-based organizations collaborating with the UC San Francisco California Preterm Birth Initiative and others on a prenatal research study designed to lower preterm birth rates, told me that the county’s highest preterm birth numbers are in Southwest Fresno — a formerly redlined, predominantly Black neighborhood of color.
Shuttered storefronts line the area west of downtown Fresno, a city with a long history of redlining, or institutionalized housing racism. Luis Sinco / Los Angeles Times via Getty Images
Black and white “women experience broadly similar climate changes, but are seeing drastically different outcomes — so something else must be at play,” said Bryttani Wooten, a Ph.D. student at the University of North Carolina at Chapel Hill who has studied racial disparities in preterm birth rates. “That something else is systemic racism, including legacies of residential segregation.”
Obstetric providers in low-income communities of color describe preterm birth as a crisis. “Preterm birth is a 24/7, 365-days-a-year public health emergency in my community,” said Nneoma Nwachuku Ojiaku, an obstetrician in Sacramento. Madeleine Wisner, who was the only midwife provider serving low-income residents in the Sacramento Valley through the state Medicaid program for seven years until recently, described something similar. “A course of maternity care where nothing abnormal happens doesn’t exist any longer in the populations I was serving,” Wisner said. She’s seen a range of birth complications — including abnormally implanted placentas, umbilical cord abnormalities, and preeclampsia — in patients who were exposed to heat, air pollution, or wildfire smoke during pregnancy.
Black doulas and midwives are a small but growing population determined to improve Black maternal health, said Maya Jackson, the founder of Mobilizing African American Mothers through Empowerment, or MAAME. She said that while Black midwives were once at the forefront of birthing health care for Black and white mothers post-slavery, their systematic exclusion from medical institutions changed that. Today, Jackson is seeking funding to do community-based research on heat impacts on people of color to make sure that their lived experiences and the impacts of policies that shape housing, green spaces, or industrial pollution in brown and black neighborhoods are documented.
“Somehow living has become a political issue,” she said.
A midwife talks with a woman and her pregnant wife in their home in Fountain Valley, California, in June 2021. In an effort to avoid racism and higher maternal mortality rates, some Black women are turning to Black midwives for care.
Sarah Reingewirtz / MediaNews Group / Los Angeles Daily News via Getty Images
Ana Bonell, a researcher at the London School of Hygiene and Tropical Medicine, studies heat and birth outcomes in western Africa and Pakistan. She said it’s difficult to conduct research on maternal climate exposure and adverse birth outcomes in most places in Africa because they often don’t have electronic health records or the equipment needed to accurately determine how far along a pregnancy is — information necessary to determine if a birth is, in fact, preterm. Instead, she looked at acute physiological changes in pregnant farmworkers and their fetuses in The Gambia, a country in West Africa where the average temperature is 83 degrees F. In 2022, she published data showing that the farmworkers exhibited a 17 percent increase in fetal stress, defined by a fetal heart rate either above 160 or below 115 beats per minute or decreased placental blood flow, for each degree Celsius of heat.
A fetal monitor checks the maternal vital signs of a woman getting ready to have a baby.
Education Images / Universal Images Group via Getty Images
“[These are] populations that have contributed almost nothing to climate change and are at [the] front lines of the climate crisis,” Bonell said. Research in Ghana, published last year, also found that exposure to temperatures 87 degrees F or higher throughout a pregnancy resulted in an 18 percent increased risk of stillbirth.
“There seems to be this myth of endless adaptation,” said Chandni Singh, a climate researcher at the Indian Institute for Human Settlements. “In tropical countries that are already very hot, there is this continuous expectation to adapt, which is not feasible. You can’t adapt to 45 C” (113 degrees F). And heat has knock-on impacts. “Heat doesn’t come alone; it comes with water scarcity and wildfires,” she said, emphasizing the need to curtail greenhouse gas emissions.
Singh has reviewed a number of heat action plans created by city and state governments globally to improve heat advisory messaging or build cooling spaces and environments. She said there is an increasing but still insufficient focus on women, particularly addressing the fact that people who are pregnant or lactating have unique heat adaptation needs.
“We know this is a problem, and certain women are affected more,” said Singh. “How do we deal with that? That’s the next challenge.”
A pregnant flood-affected woman carries her child as she walks near her tent at a makeshift camp along a railway track in India’s Punjab province in September 2022.
Arif Ali / AFP via Getty Images
While research has established the link between heat and preterm birth, the next steps are to figure out how it happens in the body, and more importantly, how to prevent it.
On an individual level, Ojiaku advises her patients, as early as possible in their pregnancies, to keep cool, stay hydrated, and limit work-related heat exposures as much as possible.
But other policies are needed to right racial inequities. In 2022, Ojiaku called on Sacramento leaders to improve public health messaging about heat risks — and to appoint a chief heat officer, akin to those in Los Angeles, Phoenix, and Miami, whose job it would be to include pregnant people as at-risk populations in heat advisories.
“We are more likely to see information on how to take care of pets during heat waves than pregnant women,” Ojiaku told me.
In addition, she said, creating green spaces such as parks in neighborhoods that have been subject to systemic racism and redlining can offer shade, cool spaces to exercise, and a buffer against air pollution.
“Sacramento is called ‘the city of trees,’ but that’s for a select few in the predominantly wealthier sections of Sacramento,” Ojiaku said. “Other areas are a concrete jungle.”
In 2023, UNICEF, the United Nations Children’s Fund, published a dossier describing measures needed to protect women and children from heat waves. It stressed prevention and preparedness, including training frontline workers to identify heat-related illness and local government adaptations such as providing cooling centers and shaded areas.
“We need to get prepared and take heat waves just as seriously as other disasters,” Ojiaku said.